

Mortality among hospitalized COVID-19 patients during surges of SARS-CoV-2 alpha (B.1.1.7) and delta (B.1.617.2) variants
- PMID: 36344540
- PMCID: PMC9640720
- DOI: 10.1038/s41598-022-23312-8
Mortality among hospitalized COVID-19 patients during surges of SARS-CoV-2 alpha (B.1.1.7) and delta (B.1.617.2) variants
Abstract
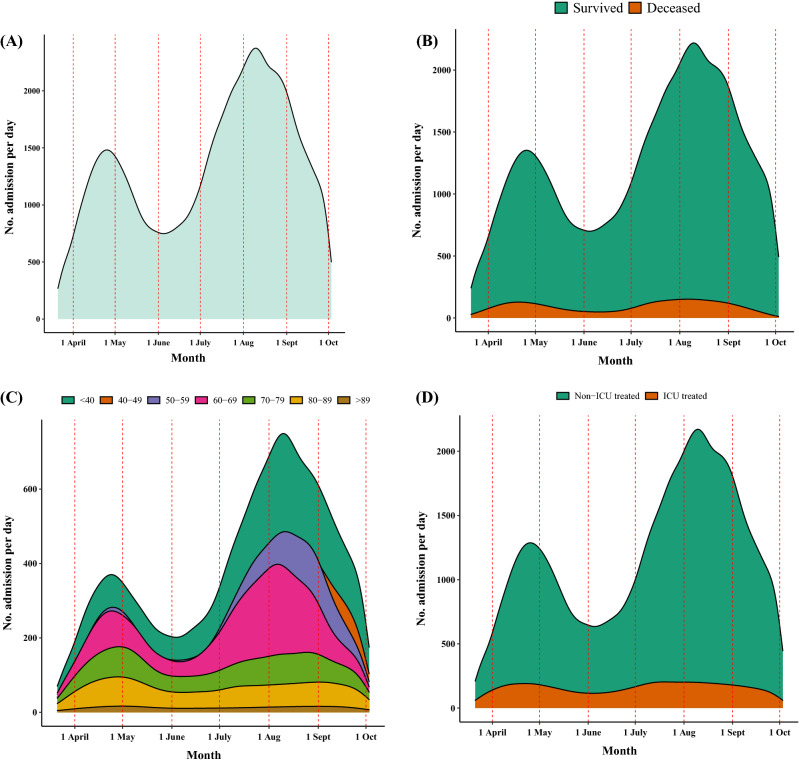
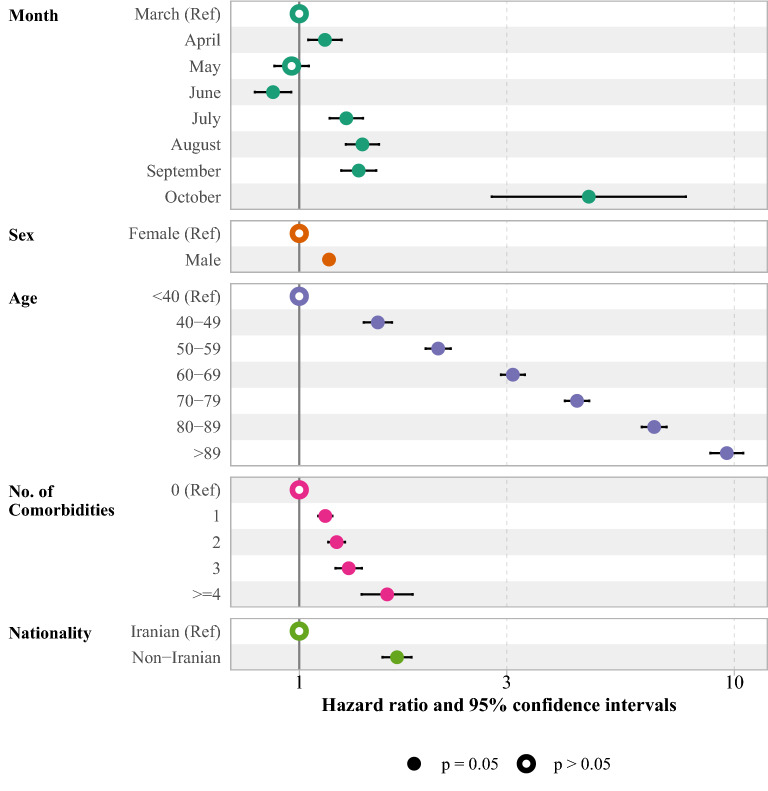
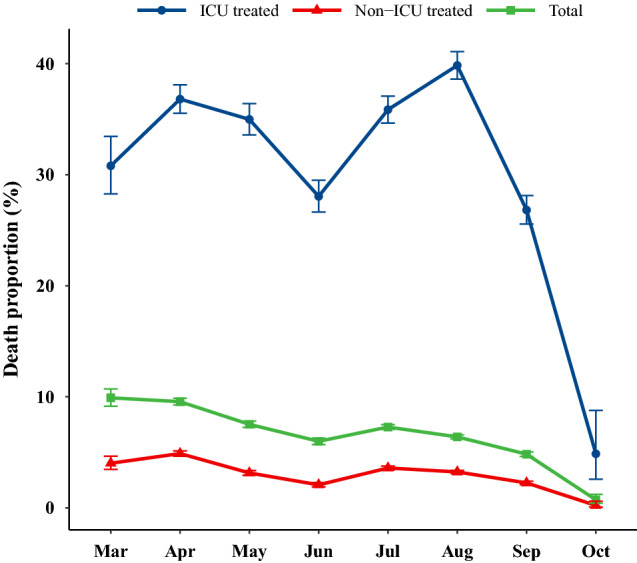
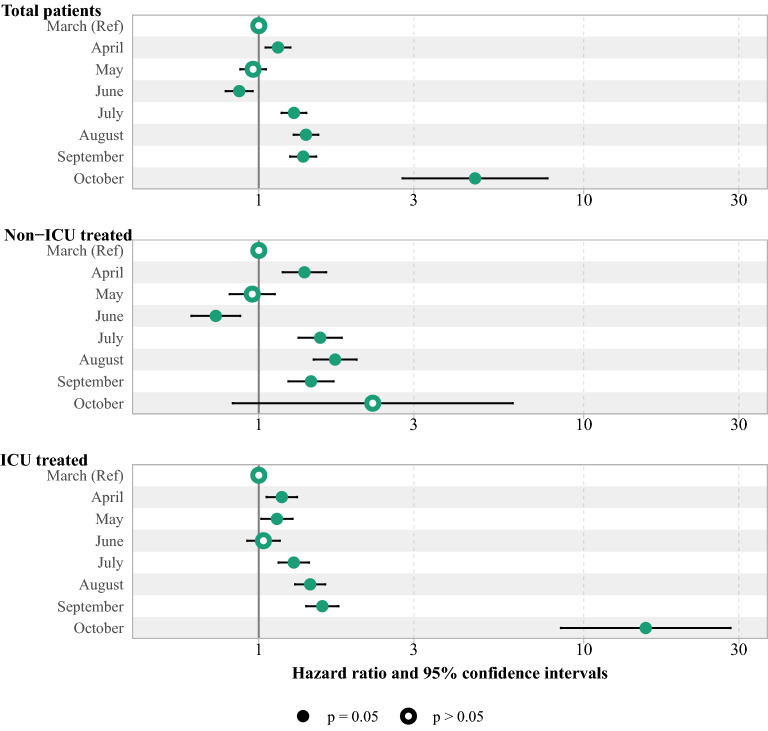
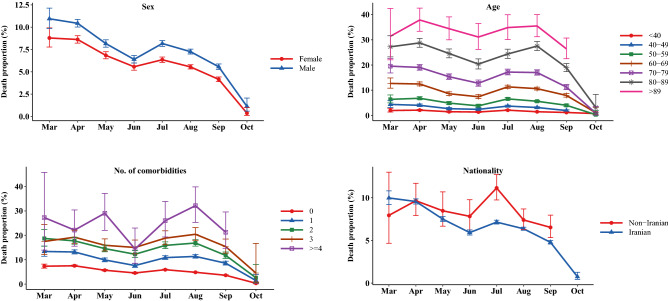
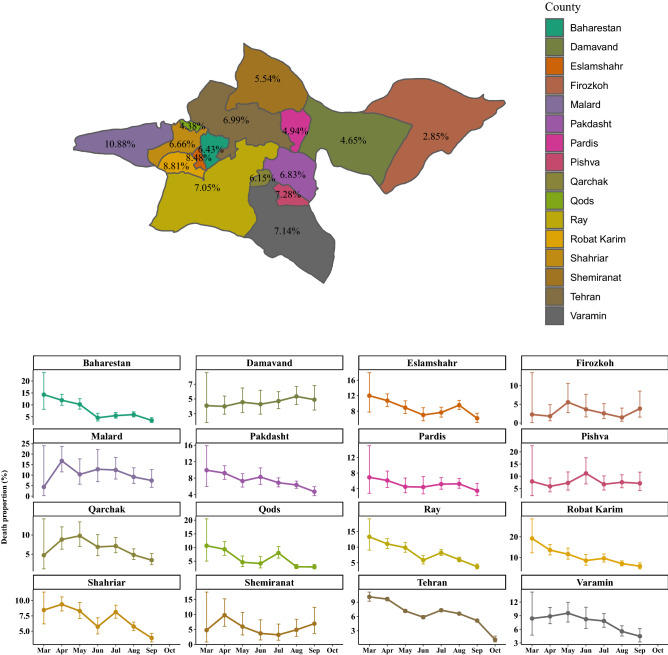
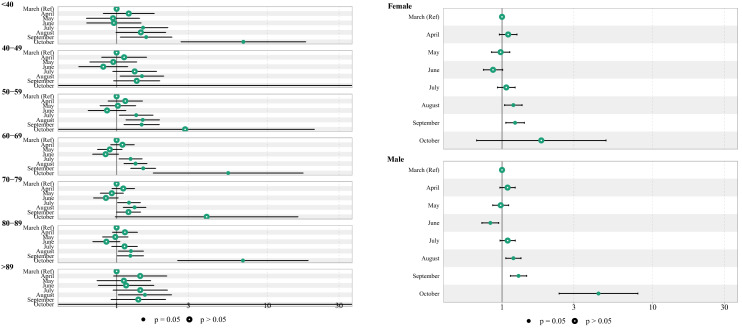
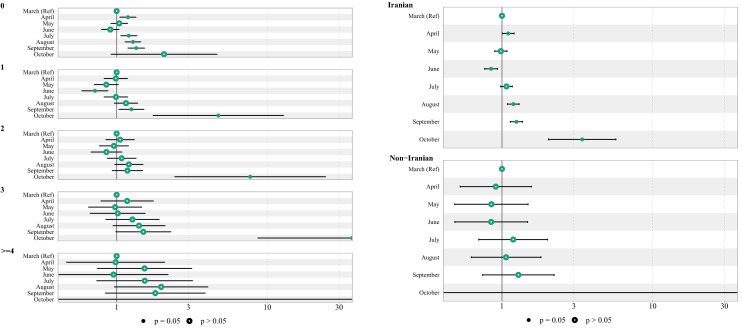
The aim of this study was to evaluate the death proportion and death risk of COVID-19 hospitalized patients over time and in different surges of COVID-19. This multi-center observational study was conducted from March 21, 2021 to October 3, 2021 which included the alpha and delta SARS-CoV-2 surges occurred in April and August in Tehran, respectively. The risk of COVID-19 death was compared in different months of admission. A total of 270,624 patients with COVID-19, of whom 6.9% died, were admitted to hospitals in Tehran province. Compared to patients admitted in March, a higher risk of COVID-19 death was observed among patients admitted to the hospital in July (HR 1.28; 95% CI 1.17, 1.40), August (HR 1.40; 95% CI 1.28, 1.52), September (HR 1.37; 95% CI 1.25, 1.50) and October (HR 4.63; 95% CI 2.77, 7.74). The ICU death proportion was 36.8% (95% CI: 35.5, 38.1) in alpha surge and increased significantly to 39.8 (95% CI 38.6, 41.1) in delta surge. The risk of COVID-19 death was significantly higher in delta surge compared to alpha surge (HR 1.22; 95% CI 1.17, 1.27). Delta surge was associated with a higher risk of death compared to alpha surge. High number of hospitalizations, a shortage of hospital beds, ICU spaces and medical supplies, poor nutritional status of hospitalized patients, and lack of the intensivist physicians or specialized nurses in the ICU were factors that contributed to the high mortality rate in the delta surge in Iran.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Trends of in-hospital and ICU mortality in COVID-19 patients over the fourth and fifth COVID-19 surges in Iran: a retrospective cohort study from Iran.Int J Qual Health Care. 2022 Aug 4;34(3):mzac063. doi: 10.1093/intqhc/mzac063. Int J Qual Health Care. 2022. PMID: 35880708 Free PMC article.
-
Clinical characteristics and outcomes of SARS-Cov-2 B.1.1.529 infections in hospitalized patients and multi-surge comparison in Louisiana.PLoS One. 2022 Oct 21;17(10):e0268853. doi: 10.1371/journal.pone.0268853. eCollection 2022. PLoS One. 2022. PMID: 36269696 Free PMC article.
-
COVID-19 in Iran: clinical presentations and outcomes in three different surges of COVID-19 infection.Virol J. 2022 Jul 26;19(1):123. doi: 10.1186/s12985-022-01846-7. Virol J. 2022. PMID: 35883172 Free PMC article.
-
Demographics, clinical characteristics, and outcomes of 27,256 hospitalized COVID-19 patients in Kermanshah Province, Iran: a retrospective one-year cohort study.BMC Infect Dis. 2022 Mar 31;22(1):319. doi: 10.1186/s12879-022-07312-7. BMC Infect Dis. 2022. PMID: 35361161 Free PMC article.
-
Clinical Characteristics and Outcomes Among Adults Hospitalized with Laboratory-Confirmed SARS-CoV-2 Infection During Periods of B.1.617.2 (Delta) and B.1.1.529 (Omicron) Variant Predominance - One Hospital, California, July 15-September 23, 2021, and December 21, 2021-January 27, 2022.MMWR Morb Mortal Wkly Rep. 2022 Feb 11;71(6):217-223. doi: 10.15585/mmwr.mm7106e2. MMWR Morb Mortal Wkly Rep. 2022. PMID: 35143466 Free PMC article.
Cited by
-
Clinical Outcome of Coronavirus Disease 2019 in Patients with Primary Antibody Deficiencies.Pathogens. 2023 Jan 9;12(1):109. doi: 10.3390/pathogens12010109. Pathogens. 2023. PMID: 36678457 Free PMC article. Review.
-
Iranian Healthcare System Response to Hospital and Intensive Care Bed Requirements During the COVID-19 Pandemic: A Cross-Sectional Study.Health Sci Rep. 2025 Apr 10;8(4):e70639. doi: 10.1002/hsr2.70639. eCollection 2025 Apr. Health Sci Rep. 2025. PMID: 40226183 Free PMC article.
-
Risk factors for mortality in hospitalized COVID-19 patients across five waves in Pakistan.Sci Rep. 2024 Aug 30;14(1):20205. doi: 10.1038/s41598-024-70662-6. Sci Rep. 2024. PMID: 39215007 Free PMC article.
-
Classification of SARS-CoV-2 sequences as recombinants via a pre-trained CNN and identification of a mathematical signature relative to recombinant feature at Spike, via interpretability.PLoS One. 2024 Aug 26;19(8):e0309391. doi: 10.1371/journal.pone.0309391. eCollection 2024. PLoS One. 2024. PMID: 39186542 Free PMC article.
-
Successive Waves of the COVID-19 Pandemic Had an Increasing Impact on Chronic Cardiovascular Patients in a Western Region of Romania.Healthcare (Basel). 2023 Apr 20;11(8):1183. doi: 10.3390/healthcare11081183. Healthcare (Basel). 2023. PMID: 37108017 Free PMC article.
References
-
- Carbonell R, et al. Mortality comparison between the first and second/third waves among 3,795 critical COVID-19 patients with pneumonia admitted to the ICU: A multicentre retrospective cohort study. Lancet Region. Health-Europe. 2021;11:100243. doi: 10.1016/j.lanepe.2021.100243. - DOI - PMC - PubMed
-
- COVID-19 Coronavirus Pandemic. COVID live - Coronavirus statistics - Worldometer. https://www.worldometers.info/coronavirus (2022).
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
