

The number of risk factors not at target is associated with cardiovascular risk in a type 2 diabetic population with albuminuria in primary cardiovascular prevention. Post-hoc analysis of the NID-2 trial
- PMID: 36344978
- PMCID: PMC9641842
- DOI: 10.1186/s12933-022-01674-7
The number of risk factors not at target is associated with cardiovascular risk in a type 2 diabetic population with albuminuria in primary cardiovascular prevention. Post-hoc analysis of the NID-2 trial
Abstract
Background: Nephropathy in Diabetes type 2 (NID-2) study is an open-label cluster randomized clinical trial that demonstrated that multifactorial intensive treatment reduces Major Adverse Cardiac Events (MACEs) and overall mortality versus standard of care in type 2 diabetic subjects with albuminuria and no history of cardiovascular disease. Aim of the present post-hoc analysis of NID- 2 study is to evaluate whether the number of risk factors on target associates with patient outcomes.
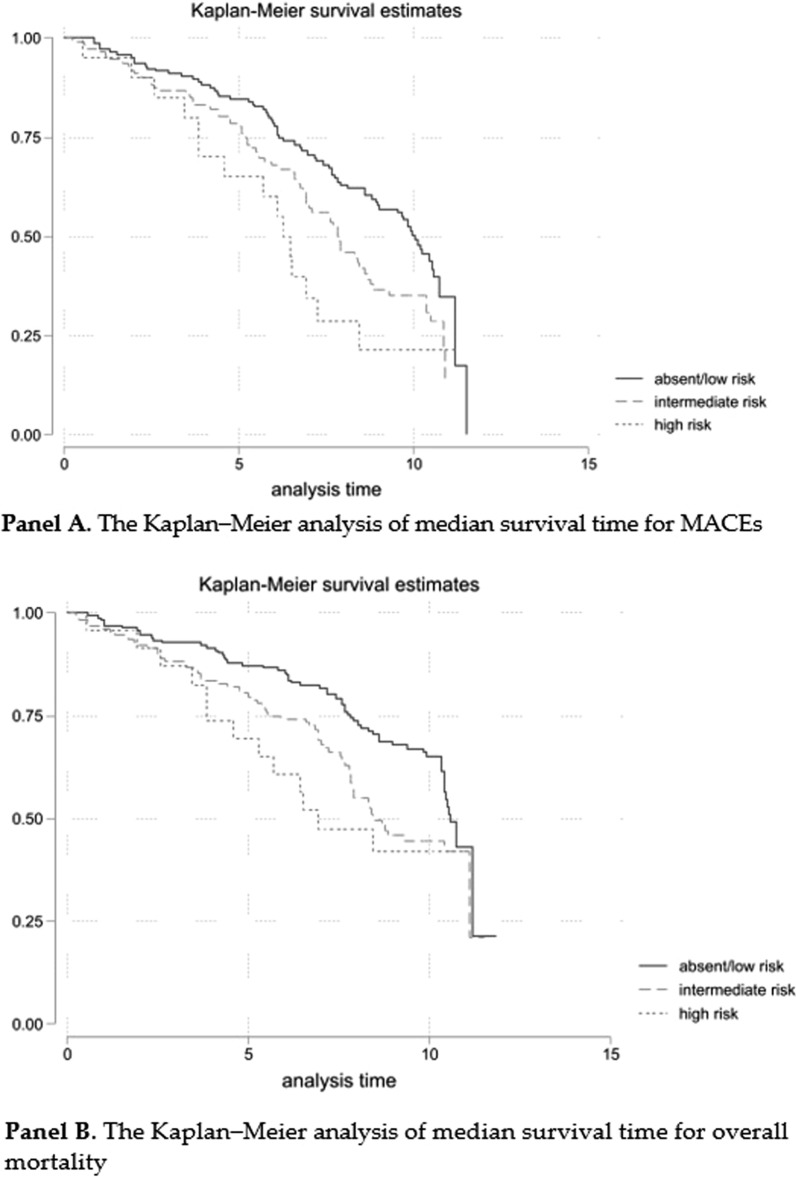
Methods: Intervention phase lasted four years and subsequent follow up for survival lasted 10 years. To the aim of this post-hoc analysis, the whole population has been divided into 3 risk groups: 0-1 risk factor (absent/low); 2-3 risk factors (intermediate); 4 risk factors (high). Primary endpoint was a composite of fatal and non-fatal MACEs, the secondary endpoint was all-cause death at the end of the follow-up phase.
Results: Absent/low risk group included 166 patients (52.4%), intermediate risk group 128 (40.4%) and high-risk group 23 (7.3%). Cox model showed a significant higher risk of MACE and death in the high-risk group after adjustment for confounding variables, including treatment arm (HR 1.91, 95% CI 1.04-3.52, P = 0.038 and 1.96, 95%CI 1.02-3.8, P = 0,045, respectively, vs absent/low risk group).
Conclusions: This post-hoc analysis of the NID-2 trial indicates that the increase in the number of risk factors at target correlates with better cardiovascular-free survival in patients with type 2 diabetes at high CV risk.
Clinical trial registration: ClinicalTrials.gov number, NCT00535925. https://clinicaltrials.gov/ct2/show/NCT00535925.
Keywords: Cardiovascular risk; Diabetes complications; Multifactorial treatment; Type 2 diabetes mellitus.
© 2022. The Author(s).
Conflict of interest statement
Ferdinando Carlo Sasso has been member of Advisory Boards for Boehringer and for Ely-Lilly and has received fees for scientific consultation and/or lectures by Jansen, Roche Diagnostics, Novo Nordisk, Sanofi, MSD, Astrazeneca. Luca De Nicola has received fees for scientific consultation and/or lectures by Astellas, AstraZeneca, Mundibiopharma and Vifor Pharma. Roberto Minutolo has been member of Advisory Boards for Amgen, Astellas, Bayer and invited speaker at meetings supported by Amgen, Astellas, Vifor Pharma. Vittorio Simeon, Raffaele Galiero, Alfredo Caturano, Paolo Chiodini, Luca Rinaldi, Teresa Salvatore, Miriam Lettieri, Riccardo Nevola, Celestino Sardu, Giovanni Docimo, Giuseppe Loffredo, Raffaele Marfella and Luigi Elio Adinolfi have no conflict of interest to disclose.
Figures
References
-
- Emerging Risk Factors Collaboration, Sarwar N, Gao P, Seshasai SR et al. Diabetes mellitus, fasting blood glucose concentration, and risk of vascular disease: a collaborative meta-analysis of 102 prospective studies [published correction appears in Lancet. 2010 Sep 18;376(9745):958. Hillage, H L [corrected to Hillege, H L]]. Lancet. 2010;375(9733):2215–2222. 10.1016/S0140-6736(10)60484-9 - PMC - PubMed
-
- Cosentino F, Grant PJ, Aboyans V et al. ESC Scientific Document Group. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur Heart J. 2020 Jan 7;41(2):255–323. 10.1093/eurheartj/ehz486. Erratum in: Eur Heart J. 2020 Dec 1;41(45):4317. PMID: 31497854. - PubMed
-
- Sasso FC, Pafundi PC, Simeon V et al. NID-2 Study Group Investigators. Efficacy and durability of multifactorial intervention on mortality and MACEs: a randomized clinical trial in type-2 diabetic kidney disease. Cardiovasc Diabetol. 2021;20(1):145. 10.1186/s12933-021-01343-1. PMID: 34271948; PMCID: PMC8285851. - PMC - PubMed
-
- American Diabetes Association. Standards of medical care in diabetes. Diabetes Care. 2005;28(Suppl 1): S4-S36. Erratum in: Diabetes Care. 2005 Apr;28(4):990. PMID: 15618112. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
