

Corticotropin-stimulated steroid profiles to predict shock development and mortality in sepsis: From the HYPRESS study
- PMID: 36345013
- PMCID: PMC9641871
- DOI: 10.1186/s13054-022-04224-5
Corticotropin-stimulated steroid profiles to predict shock development and mortality in sepsis: From the HYPRESS study
Abstract
Rationale: Steroid profiles in combination with a corticotropin stimulation test provide information about steroidogenesis and its functional reserves in critically ill patients.
Objectives: We investigated whether steroid profiles before and after corticotropin stimulation can predict the risk of in-hospital death in sepsis.
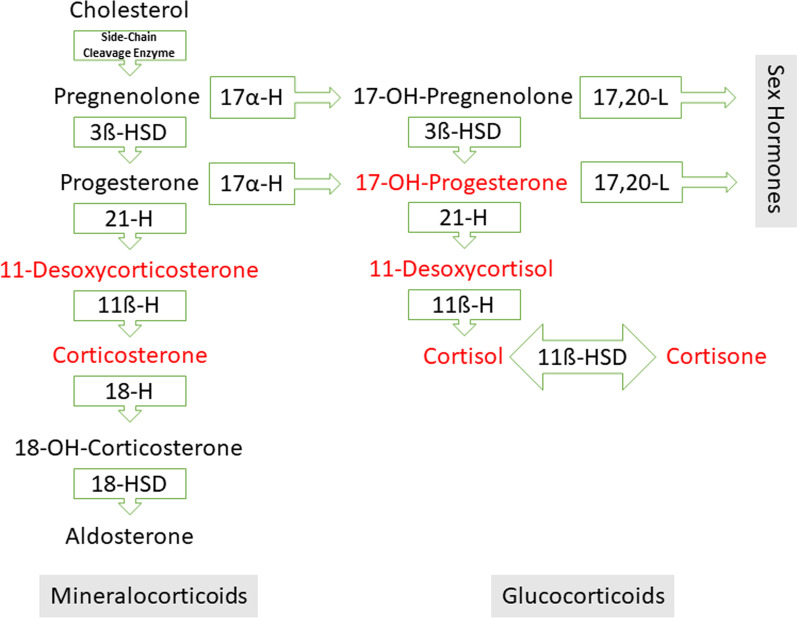
Methods: An exploratory data analysis of a double blind, randomized trial in sepsis (HYPRESS [HYdrocortisone for PRevention of Septic Shock]) was performed. The trial included adult patients with sepsis who were not in shock and were randomly assigned to placebo or hydrocortisone treatment. Corticotropin tests were performed in patients prior to randomization and in healthy subjects. Cortisol and precursors of glucocorticoids (17-OH-progesterone, 11-desoxycortisol) and mineralocorticoids (11-desoxycorticosterone, corticosterone) were analyzed using the multi-analyte stable isotope dilution method (LC-MS/MS). Measurement results from healthy subjects were used to determine reference ranges, and those from placebo patients to predict in-hospital mortality.
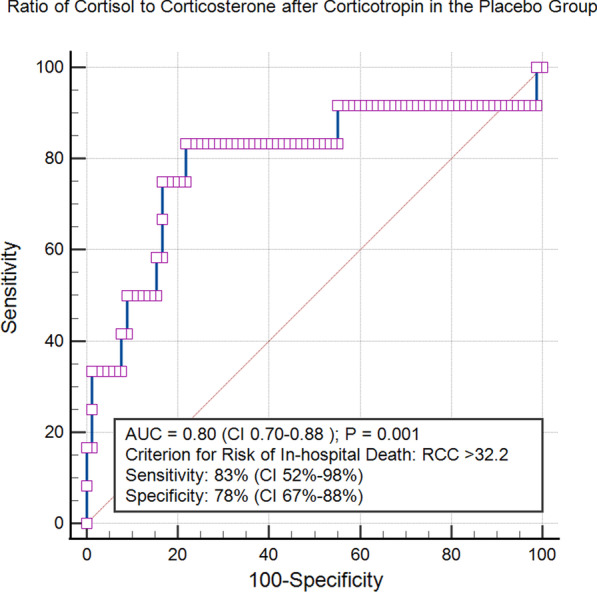
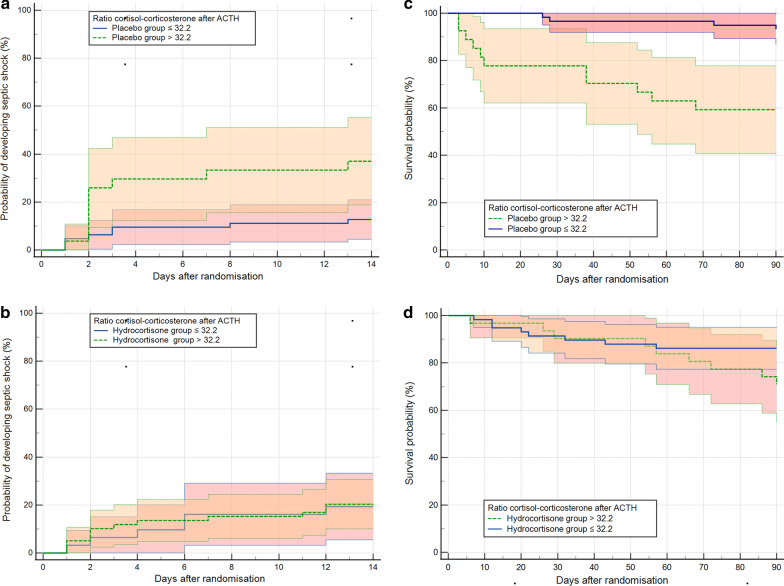
Measurements and main results: Corticotropin tests from 180 patients and 20 volunteers were included. Compared to healthy subjects, patients with sepsis had elevated levels of 11-desoxycorticosterone and 11-desoxycortisol, consistent with activation of both glucocorticoid and mineralocorticoid pathways. After stimulation with corticotropin, the cortisol response was subnormal in 12% and the corticosterone response in 50% of sepsis patients. In placebo patients (n = 90), a corticotropin-stimulated cortisol-to-corticosterone ratio > 32.2 predicted in-hospital mortality (AUC 0.8 CI 0.70-0.88; sensitivity 83%; and specificity 78%). This ratio also predicted risk of shock development and 90-day mortality.
Conclusions: In this exploratory analysis, we found that in sepsis mineralocorticoid steroidogenesis was more frequently impaired than glucocorticoid steroidogenesis. The corticotropin-stimulated cortisol-to-corticosterone ratio predicts the risk of in-hospital death. Trial registration Clinical trial registered with www.
Clinicaltrials: gov Identifier: NCT00670254. Registered 1 May 2008, https://clinicaltrials.gov/ct2/show/NCT00670254 .
Keywords: Corticosterone; Hospital mortality; Hydrocortisone; Mass spectrometry; Sepsis; Septic; Shock; Steroids.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
The authors declare no conflict of interest.
Figures


References
-
- Van den Berghe G, Téblick A, Langouche L, Gunst J. The hypothalamus-pituitary-adrenal axis in sepsis- and hyperinflammation-induced critical illness: Gaps in current knowledge and future translational research directions. EBioMedicine. 2022;84:104284. doi: 10.1016/j.ebiom.2022.104284. - DOI - PMC - PubMed
-
- Annane D, Pastores SM, Arlt W, Balk RA, Beishuizen A, Briegel J, Carcillo J, Christ-Crain M, Cooper MS, Marik PE, et al. Critical illness-related corticosteroid insufficiency (CIRCI): a narrative review from a Multispecialty Task Force of the Society of Critical Care Medicine (SCCM) and the European Society of Intensive Care Medicine (ESICM) Intensive Care Med. 2017;43(12):1781–1792. doi: 10.1007/s00134-017-4914-x. - DOI - PubMed
-
- Peeters B, Meersseman P, Vander Perre S, Wouters PJ, Debaveye Y, Langouche L, Van den Berghe G. ACTH and cortisol responses to CRH in acute, subacute, and prolonged critical illness: a randomized, double-blind, placebo-controlled, crossover cohort study. Intensive Care Med. 2018;44(12):2048–2058. doi: 10.1007/s00134-018-5427-y. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
