

The diagnostic role of T wave morphology biomarkers in congenital and acquired long QT syndrome: A systematic review
- PMID: 36345173
- PMCID: PMC9833360
- DOI: 10.1111/anec.13015
The diagnostic role of T wave morphology biomarkers in congenital and acquired long QT syndrome: A systematic review
Abstract
Introduction: QTc prolongation is key in diagnosing long QT syndrome (LQTS), however 25%-50% with congenital LQTS (cLQTS) demonstrate a normal resting QTc. T wave morphology (TWM) can distinguish cLQTS subtypes but its role in acquired LQTS (aLQTS) is unclear.
Methods: Electronic databases were searched using the terms "LQTS," "long QT syndrome," "QTc prolongation," "prolonged QT," and "T wave," "T wave morphology," "T wave pattern," "T wave biomarkers." Whole text articles assessing TWM, independent of QTc, were included.
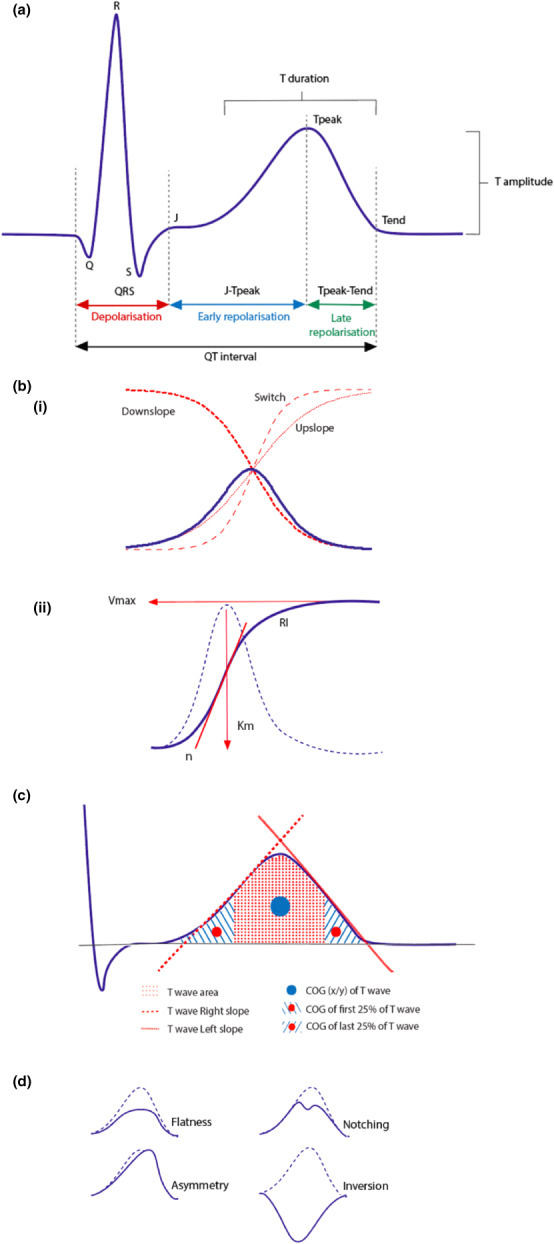
Results: Seventeen studies met criteria. TWM measurements included T-wave amplitude, duration, magnitude, Tpeak-Tend, QTpeak, left and right slope, center of gravity (COG), sigmoidal and polynomial classifiers, repolarizing integral, morphology combination score (MCS) and principal component analysis (PCA); and vectorcardiographic biomarkers. cLQTS were distinguished from controls by sigmoidal and polynomial classifiers, MCS, QTpeak, Tpeak-Tend, left slope; and COG x axis. MCS detected aLQTS more significantly than QTc. Flatness, asymmetry and notching, J-Tpeak; and Tpeak-Tend correlated with QTc in aLQTS. Multichannel block in aLQTS was identified by early repolarization (ERD30% ) and late repolarization (LRD30% ), with ERD reflecting hERG-specific blockade. Cardiac events were predicted in cLQTS by T wave flatness, notching, and inversion in leads II and V5 , left slope in lead V6 ; and COG last 25% in lead I. T wave right slope in lead I and T-roundness achieved this in aLQTS.
Conclusion: Numerous TWM biomarkers which supplement QTc assessment were identified. Their diagnostic capabilities include differentiation of genotypes, identification of concealed LQTS, differentiating aLQTS from cLQTS; and determining multichannel versus hERG channel blockade.
Keywords: ECG biomarkers; LQTS; T wave morphology; acquired long QT syndrome; congenital long QT syndrome; sudden cardiac death.
© 2022 The Authors. Annals of Noninvasive Electrocardiology published by Wiley Periodicals LLC.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


References
-
- Al‐Khatib, S. M. , Stevenson, W. G. , Ackerman, M. J. , Bryant, W. J. , Callans, D. J. , Curtis, A. B. , Deal, B. J. , Dickfield, T. , Field, M. E. , Fonarow, G. C. , Gillis, A. M. , Granger, C. B. , Hammill, S. C. , Hlatky, M. A. , Joglar, J. A. , Kay, G. N. , Matlock, D. D. , Myerburg, R. J. , & Page, R. L. (2018). 2017 AHA/ACC/HRS guideline for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: A report from of the American College of Cardiology/American Heart Association task force on clinical practice guidelines and the heart rhythm society. Circulation, 138, e272–e391. 10.1161/CIR.0000000000000549 - DOI - PubMed
-
- Anderson, M. P. , Xue, J. Q. , Graff, C. , Hardahl, T. B. , Toft, E. , Kanters, J. K. , Christiansen, M. , Jensen, H. K. , & Struijik, J. J. (2007). A robust method for quantification of IKr‐related T‐wave morphology abnormalities. Computing in Cardiology, 34, 341,344. 10.1109/CIC.2007.4745491 - DOI
-
- Attia, Z. I. , Sugrue, A. , Asirvatham, S. J. , Ackerman, M. J. , Kapa, S. , & Friedman, P. A. (2018). Noninvasive assessment of dofetilide plasma concentration using a deep learning (neural network) analysis of the surface electrocardiogram: A proof of concept study. PLoS ONE, 13(8), e0201059. 10.1371/journal.pone.0201059 - DOI - PMC - PubMed
-
- Barsheshet, A. , Peterson, D. R. , Moss, A. J. , Schwartz, P. J. , Kaufman, E. S. , McNitt, S. , Polonsky, S. , Buber, J. , Zareba, W. , Robinson, J. L. , Ackerman, M. J. , Benhorin, J. , Towbin, J. A. , Vincent, G. M. , Zhang, L. , & Goldenberg, I. (2011). Genotype‐specific QT correction for heart rate and the risk of life‐threatening cardiac events in adolescents with congenital long‐QT syndrome. Heart Rhythm, 8(8), 1207–1213. 10.1016/j.hrthm.2011.03.009 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
