

A Rare Case of MRSA Pericarditis with Expanding, Purulent Pericardial Effusion Leading to Uremic Kidney Failure from a Right, Necrotic Toe
- PMID: 36345478
- PMCID: PMC9637036
- DOI: 10.1155/2022/7041740
A Rare Case of MRSA Pericarditis with Expanding, Purulent Pericardial Effusion Leading to Uremic Kidney Failure from a Right, Necrotic Toe
Abstract
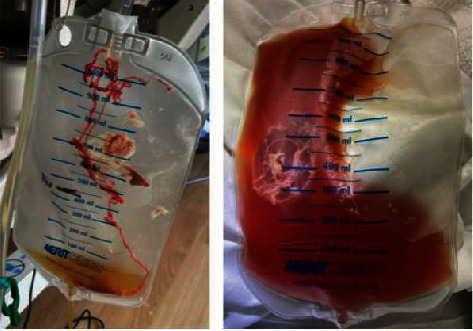
Purulent pericarditis is an extremely rare entity with only a few reported cases so far. This condition deserves prompt diagnosis because of its significant mortality rate if left untreated. A 76-year-old man with a past medical history of coronary artery disease (CAD) with percutaneous coronary intervention (PCI) to the left anterior descending artery (LAD) and right circumflex artery (RCA), ischemic cardiomyopathy with moderately reduced ejection fraction (EF 45-50%), peripheral artery disease (PAD), COVID-19 pneumonia complicated by fibrotic lung disease (on 3 liters of home oxygen), type-2 diabetes mellitus (T2DM), hypertension (HTN), hyperlipidemia (HLD), and chronic kidney disease (CKD) stage III presented with complaints of pleuritic chest pain and shortness of breath. On hospital day 1, he was afebrile and hemodynamically stable with physical exam remarkable for bibasilar crackles and dry gangrene of his right first toe. He developed progressive altered mental status, hypotension, oliguric renal failure, and respiratory distress on hospital day 6. On exam at this time, he had an elevated jugular venous distension (JVD) of 12-14 cm water, pericardial friction rub with decreased heart sounds, and orthopnea; all were consistent with cardiac tamponade clinically. An electrocardiogram (EKG) showed new ST elevations in leads I, II, and aVL with ST depression in aVR and V1 with only mild elevation in troponin I to 0.07 ng/mL. A transthoracic echocardiogram (TTE) was done on hospital day 7 and showed a moderate sized pericardial effusion with inferior vena cava (IVC) enlargement but no atrial collapse, ventricular collapse, IVC collapse, or respiratory variation in the mitral and tricuspid inflow velocities. Blood cultures grew methicillin-resistant Staphylococcus aureus (MRSA) on hospital day 6, and he was started on intravenous (IV) vancomycin. The differential diagnosis for his enlarging pericardial effusion included purulent pericarditis, uremic pericarditis, or hemorrhagic effusion. He had urgent diagnostic and therapeutic pericardiocentesis with removal of 350 milliliters of fluid. The pericardial fluid was cloudy, tan-brown with a gram stain showing gram-positive cocci in clusters and cultures growing MRSA, which confirmed the diagnosis of purulent pericarditis secondary to MRSA infection. After the pericardiocentesis, his blood pressure, respiratory distress, and renal failure improved. The source of the bacteremia was from osteomyelitis of his gangrenous, right toe with bone biopsy growing both MRSA and Streptococcus anginosus. He underwent toe amputation for definitive source control. He was discharged on hospital day 24 with a plan to complete 6 weeks of IV vancomycin.
Copyright © 2022 Justin Brilliant et al.
Conflict of interest statement
The authors report no conflict of interest.
Figures



Similar articles
-
Methicillin-resistant Staphylococcus aureus pericarditis causing cardiac tamponade.IDCases. 2019 Aug 1;18:e00613. doi: 10.1016/j.idcr.2019.e00613. eCollection 2019. IDCases. 2019. PMID: 31453103 Free PMC article.
-
A Complex Case of Idiopathic Purulent Pericarditis in an Immunocompetent Adult.Cureus. 2023 Oct 12;15(10):e46930. doi: 10.7759/cureus.46930. eCollection 2023 Oct. Cureus. 2023. PMID: 37841995 Free PMC article.
-
A Case Report of Methicillin-Resistant Staphylococcus aureus-Related Pericardial Empyema: A Deadly Cardiac Risk.Cureus. 2024 Oct 2;16(10):e70684. doi: 10.7759/cureus.70684. eCollection 2024 Oct. Cureus. 2024. PMID: 39493020 Free PMC article.
-
Massive purulent pericardial effusion presenting as atrial fibrillation with rapid rate: case report and review of the literature.Am J Case Rep. 2014 Nov 19;15:504-7. doi: 10.12659/AJCR.889851. Am J Case Rep. 2014. PMID: 25407956 Free PMC article. Review.
-
Purulent pericarditis secondary to community-acquired, methicillin-resistant Staphylococcus aureus in previously healthy children. A sign of the times?Ann Am Thorac Soc. 2013 Jun;10(3):235-8. doi: 10.1513/AnnalsATS.201211-104BC. Ann Am Thorac Soc. 2013. PMID: 23802820 Review.
Cited by
-
Recurrent Idiopathic Methicillin-sensitive Staphylococcus aureus Pericarditis in a Patient with SARS-CoV-2 Infection and Septic Bacteremia: Case Report.US Cardiol. 2025 Feb 10;19:e03. doi: 10.15420/usc.2024.43. eCollection 2025. US Cardiol. 2025. PMID: 40017720 Free PMC article.
-
Severe pneumonia combined with septic shock caused by community-acquired methicillin-resistant Staphylococcus aureus treated with veno-venous ECMO: A case report.Medicine (Baltimore). 2025 Mar 28;104(13):e41627. doi: 10.1097/MD.0000000000041627. Medicine (Baltimore). 2025. PMID: 40153769 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
