

Effect of Weight Loss on Early Left Atrial Myopathy in People With Obesity But No Established Cardiovascular Disease
- PMID: 36346054
- PMCID: PMC9750071
- DOI: 10.1161/JAHA.122.026023
Effect of Weight Loss on Early Left Atrial Myopathy in People With Obesity But No Established Cardiovascular Disease
Abstract
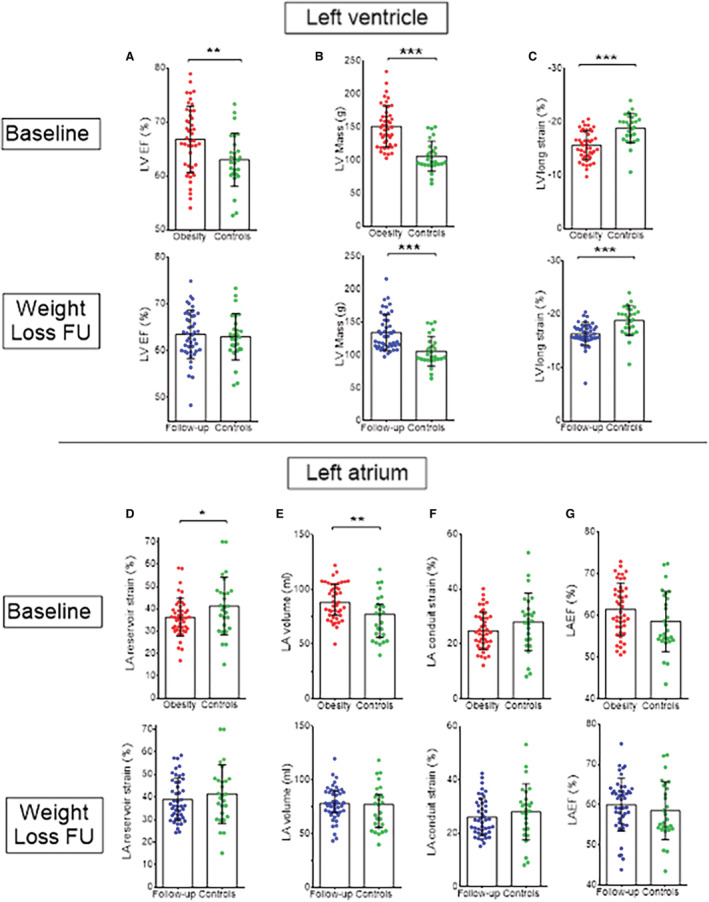
Background Obesity is associated with left atrial (LA) remodeling (ie, dilatation and dysfunction) which is an independent determinant of future cardiovascular events. We aimed to assess whether LA remodeling is present in obesity even in individuals without established cardiovascular disease and whether it can be improved by intentional weight loss. Methods and Results Forty-five individuals with severe obesity without established cardiovascular disease (age, 45±11 years; body mass index; 39.1±6.7 kg/m2; excess body weight, 51±18 kg) underwent cardiac magnetic resonance for quantification of LA and left ventricular size and function before and at a median of 373 days following either a low glycemic index diet (n=28) or bariatric surgery (n=17). Results were compared with those obtained in 27 normal-weight controls with similar age and sex. At baseline, individuals with obesity displayed reduced LA reservoir function (a marker of atrial distensibility), and a higher mass and LA maximum volume (all P<0.05 controls) but normal LA emptying fraction. On average, weight loss led to a significant reduction of LA maximum volume and left ventricular mass (both P<0.01); however, significant improvement of the LA reservoir function was only observed in those at the upper tertile of weight loss (≥47% excess body weight loss). Following weight loss, we found an average residual increase in left ventricular mass compared with controls but no residual significant differences in LA maximum volume and strain function (all P>0.05). Conclusions Obesity is linked to subtle LA myopathy in the absence of overt cardiovascular disease. Only larger volumes of weight loss can completely reverse the LA myopathic phenotype.
Keywords: left atrial myopathy; obesity; reservoir strain; weight loss.
Figures


References
-
- Eaton CB, Pettinger M, Rossouw J, Martin LW, Foraker R, Quddus A, Liu S, Wampler NS, Hank Wu WC, Manson JE, et al. Risk factors for incident hospitalized heart failure with preserved versus reduced ejection fraction in a multiracial cohort of postmenopausal women. Circ Heart Fail. 2016;9:e002883. doi: 10.1161/CIRCHEARTFAILURE.115.002883 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
