

Evaluation of MRI-only based online adaptive radiotherapy of abdominal region on MR-linac
- PMID: 36347050
- PMCID: PMC10018672
- DOI: 10.1002/acm2.13838
Evaluation of MRI-only based online adaptive radiotherapy of abdominal region on MR-linac
Abstract
Purpose: A hybrid magnetic resonance linear accelerator (MRL) can perform magnetic resonance imaging (MRI) with high soft-tissue contrast to be used for online adaptive radiotherapy (oART). To obtain electron densities needed for the oART dose calculation, a computed tomography (CT) is often deformably registered to MRI. Our aim was to evaluate an MRI-only based synthetic CT (sCT) generation as an alternative to the deformed CT (dCT)-based oART in the abdominal region.
Methods: The study data consisted of 57 patients who were treated on a 0.35 T MRL system mainly for abdominal tumors. Simulation MRI-CT pairs of 43 patients were used for training and validation of a prototype convolutional neural network sCT-generation algorithm, based on HighRes3DNet, for the abdominal region. For remaining test patients, sCT images were produced from simulation MRIs and daily MRIs. The dCT-based plans were re-calculated on sCT with identical calculation parameters. The sCT and dCT were compared in terms of geometric agreement and calculated dose.
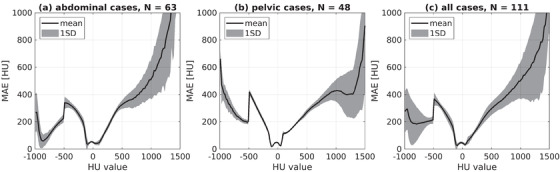
Results: The mean and one standard deviation of the geometric agreement metrics over dCT-sCT-pairs were: mean error of 8 ± 10 HU, mean absolute error of 49 ± 10 HU, and Dice similarity coefficient of 55 ± 12%, 60 ± 5%, and 82 ± 15% for bone, fat, and lung tissues, respectively. The dose differences between the sCT and dCT-based dose for planning target volumes were 0.5 ± 0.9%, 0.6 ± 0.8%, and 0.5 ± 0.8% at D2% , D50% , and D98% in physical dose and 0.8 ± 1.4%, 0.8 ± 1.2%, and 0.6 ± 1.1% in biologically effective dose (BED). For organs-at-risk, the dose differences of all evaluated dose-volume histogram points were within [-4.5%, 7.8%] and [-1.1 Gy, 3.5 Gy] in both physical dose and BED.
Conclusions: The geometric agreement metrics were within typically reported values and most average relative dose differences were within 1%. Thus, an MRI-only sCT-based approach is a promising alternative to the current clinical practice of the abdominal oART on MRL.
Keywords: MR-linac; MRI-only; online adaptive radiotherapy; synthetic CT.
© 2022 The Authors. Journal of Applied Clinical Medical Physics published by Wiley Periodicals, LLC on behalf of The American Association of Physicists in Medicine.
Conflict of interest statement
Nils Lundahl, Rickard Cronholm, and Carl Siversson are employed at Spectronic Medical AB. The authors have no other conflicts of interest to declare.
Figures


References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
