The Impact of Fractional Flow Reserve on Clinical Outcomes after Coronary Artery Bypass Grafting: A Meta-analysis
- PMID: 36348504
- PMCID: PMC9733408
- DOI: 10.5090/jcs.22.072
The Impact of Fractional Flow Reserve on Clinical Outcomes after Coronary Artery Bypass Grafting: A Meta-analysis
Abstract
Background: This meta-analysis was conducted to evaluate the effect of fractional flow reserve (FFR) on clinical outcomes after coronary artery bypass grafting (CABG).
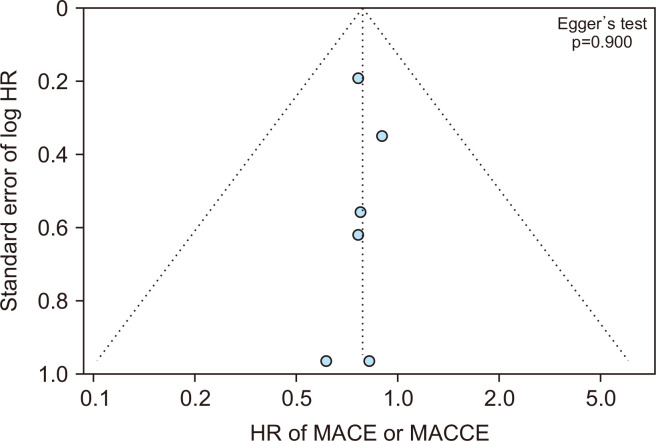
Methods: Five online databases were searched for studies that (1) enrolled patients who underwent isolated CABG or CABG with aortic valve replacement and (2) demonstrated the effect of an FFR-guided strategy on major adverse cardiac events (MACE) after surgery based on a randomized controlled trial or adjusted analysis. MACE included cardiac death, acute myocardial infarction (MI), and repeated revascularization. The primary outcomes were all MACE outcomes and a composite of all-cause death and MI, and the secondary outcomes were the individual MACE outcomes. Publication bias was assessed using a funnel plot and the Egger test.
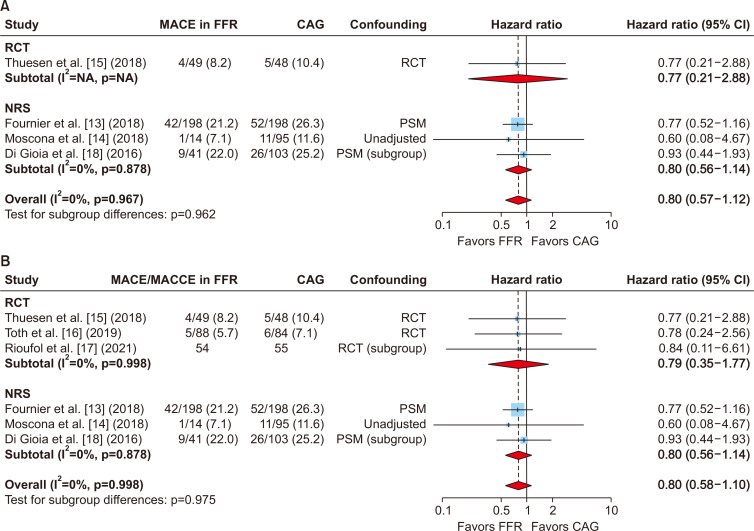
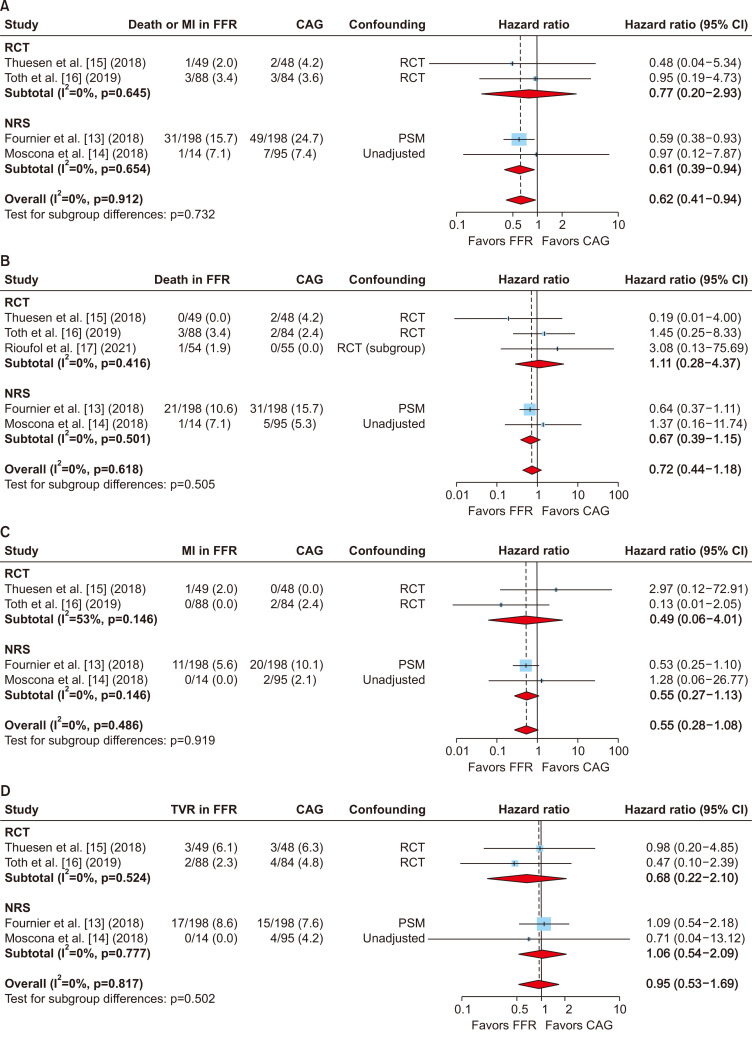
Results: Six articles (3 randomized and 3 non-randomized studies: n=1,027) were selected. MACE data were extracted from 4 studies. The pooled analyses showed that the risk of MACE was not significantly different between patients who underwent FFR-guided CABG and those who underwent angiography-guided CABG (hazard ratio [HR], 0.80; 95% CI, 0.57-1.12). However, the risk of the composite of death or MI was significantly lower in patients undergoing FFR-guided CABG (HR, 0.62; 95% CI, 0.41-0.94). The individual MACE outcomes were not significantly different between FFR-guided and angiography-guided CABG.
Conclusion: FFR-guided CABG might be beneficial in terms of the composite outcome of death or MI compared with angiography-guided CABG although data are limited.
Keywords: Coronary artery bypass grafting; Fractional flow reserve; Meta-analysis; Statistics.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures

Similar articles
-
Coronary Artery Bypass Grafting or Fractional Flow Reserve-Guided Percutaneous Coronary Intervention in Diabetic Patients With Multivessel Disease.Circ Cardiovasc Interv. 2020 Oct;13(10):e009157. doi: 10.1161/CIRCINTERVENTIONS.120.009157. Epub 2020 Oct 12. Circ Cardiovasc Interv. 2020. PMID: 33040579
-
The role of fractional flow reserve in coronary artery bypass graft surgery: a meta-analysis.Interact Cardiovasc Thorac Surg. 2020 May 1;30(5):671-678. doi: 10.1093/icvts/ivaa006. Interact Cardiovasc Thorac Surg. 2020. PMID: 32167555 Review.
-
Fractional Flow Reserve Versus Angiographically-Guided Coronary Artery Bypass Grafting.J Am Coll Cardiol. 2018 Dec 4;72(22):2732-2743. doi: 10.1016/j.jacc.2018.09.043. J Am Coll Cardiol. 2018. PMID: 30497559 Clinical Trial.
-
Fractional Flow Reserve-Guided PCI or Coronary Bypass Surgery for 3-Vessel Coronary Artery Disease: 3-Year Follow-Up of the FAME 3 Trial.Circulation. 2023 Sep 19;148(12):950-958. doi: 10.1161/CIRCULATIONAHA.123.065770. Epub 2023 Aug 21. Circulation. 2023. PMID: 37602376 Clinical Trial.
-
FFR-guided versus coronary angiogram-guided CABG: A review and meta-analysis of prospective randomized controlled trials.J Card Surg. 2020 Oct;35(10):2785-2793. doi: 10.1111/jocs.14880. Epub 2020 Jul 22. J Card Surg. 2020. PMID: 32697006
References
-
- Toth GG, Toth B, Johnson NP, et al. Revascularization decisions in patients with stable angina and intermediate lesions: results of the international survey on interventional strategy. Circ Cardiovasc Interv. 2014;7:751–9. doi: 10.1161/CIRCINTERVENTIONS.114.001608. https://doi.org/10.1161/CIRCINTERVENTIONS.114.001608. - DOI - PubMed
-
- Toth G, Hamilos M, Pyxaras S, et al. Evolving concepts of angiogram: fractional flow reserve discordances in 4000 coronary stenoses. Eur Heart J. 2014;35:2831–8. doi: 10.1093/eurheartj/ehu094. https://doi.org/10.1093/eurheartj/ehu094. - DOI - PubMed
-
- Pijls NH, van Schaardenburgh P, Manoharan G, et al. Percutaneous coronary intervention of functionally nonsignificant stenosis: 5-year follow-up of the DEFER Study. J Am Coll Cardiol. 2007;49:2105–11. doi: 10.1016/j.jacc.2007.01.087. https://doi.org/10.1016/j.jacc.2007.01.087. - DOI - PubMed
-
- Tonino PA, De Bruyne B, Pijls NH, et al. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N Engl J Med. 2009;360:213–24. doi: 10.1056/NEJMoa0807611. https://doi.org/10.1056/NEJMoa0807611. - DOI - PubMed
-
- Ciccarelli G, Barbato E, Toth GG, et al. Angiography versus hemodynamics to predict the natural history of coronary stenoses: fractional flow reserve versus angiography in multivessel evaluation 2 substudy. Circulation. 2018;137:1475–85. doi: 10.1161/CIRCULATIONAHA.117.028782. https://doi.org/10.1161/CIRCULATIONAHA.117.028782. - DOI - PubMed
LinkOut - more resources
Full Text Sources