

External Lumbar Drainage for Refractory Intracranial Hypertension in Traumatic Brain Injury: A Systematic Review
- PMID: 36348893
- PMCID: PMC9637378
- DOI: 10.7759/cureus.30033
External Lumbar Drainage for Refractory Intracranial Hypertension in Traumatic Brain Injury: A Systematic Review
Abstract
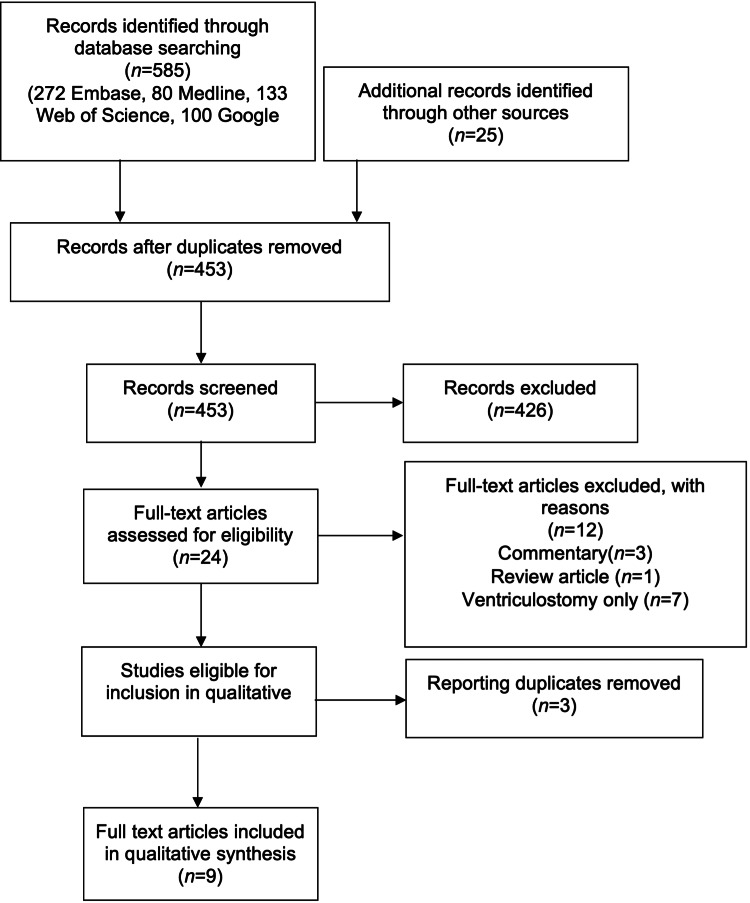
Considerable variation exists in the clinical practice of cerebrospinal fluid diversion for medically refractory intracranial hypertension in patients with acute traumatic brain injury (TBI), which is achievable via lumbar or ventricular drainage. This systematic review sought to compile the available evidence for the efficacy and safety of the use of lumbar drains for intracranial pressure (ICP) control. A systematic review of the literature was performed with the search and data extraction performed by two reviewers independently in duplicate. Nine independent studies were identified, enrolling 230 patients, 159 with TBI. Efficacy for ICP control was observed across all studies, with immediate and sustained effect, reducing medical therapy requirements. Lumbar drainage with medical therapy appears effective when used alone and as an adjunct to ventricular drainage. Safety reporting varied in quality. Clinical or radiological incidents of cerebral herniation (with an unclear relationship to lumbar drainage) were observed in 14/230 patients resulting in one incident of morbidity without adverse patient outcome. The available data is generally poor in quality and volume, but supportive of the efficacy of lumbar drainage for ICP control. Few reports of adverse outcomes are suggestive of, but are insufficient to confirm, the safety of use in the appropriate patient and clinical setting. Further large prospective observational studies are required to generate sufficient support of an acceptable safety profile.
Keywords: cerebrospinal fluid drainage; critical care; intracranial hypertension; neurosurgery; traumatic brain injury.
Copyright © 2022, Stevens et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Guidelines for the management of severe traumatic brain injury, fourth edition. Carney N, Totten AM, O'Reilly C, et al. Neurosurgery. 2017;80:6–15. - PubMed
-
- Observations on the structure and functions of the nervous system, illustrated with tables. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5545466/ Lond Med J. 1783;4:113–135.
-
- An account of the appearances observed in the dissection of two of the three individuals presumed to have perished in the storm of the 3rd, and whose bodies were discovered in the vicinity of Leith on the morning of the 4th November 1821 with some reflections on the pathology of the brain: part I. Kellie G. https://europepmc.org/article/pmc/5405298 Transac Med Chir Soc Edinburgh. 1824;1:84–169. - PMC - PubMed
-
- Intermittent versus continuous cerebrospinal fluid drainage management in adult severe traumatic brain injury: assessment of intracranial pressure burden. Nwachuku EL, Puccio AM, Fetzick A, Scruggs B, Chang YF, Shutter LA, Okonkwo DO. Neurocrit Care. 2014;20:49–53. - PubMed
-
- Primary external ventricular drainage catheter versus intraparenchymal ICP monitoring: outcome analysis. Bales JW, Bonow RH, Buckley RT, Barber J, Temkin N, Chesnut RM. Neurocrit Care. 2019;31:11–21. - PubMed
Publication types
LinkOut - more resources
Full Text Sources