

Serum Soluble Scavenger Receptor A Levels are Associated with Delayed Cerebral Ischemia and Poor Clinical Outcome After Aneurysmal Subarachnoid Hemorrhage: A Prospective Observational Study
- PMID: 36349344
- PMCID: PMC9637348
- DOI: 10.2147/NDT.S387487
Serum Soluble Scavenger Receptor A Levels are Associated with Delayed Cerebral Ischemia and Poor Clinical Outcome After Aneurysmal Subarachnoid Hemorrhage: A Prospective Observational Study
Abstract
Objective: Scavenger receptor A (SRA), a pattern recognition molecule, is implicated in immune response after acute brain injury. We strived to identify serum soluble SRA (sSRA) as a potential biomarker of prognosis after aneurysmal subarachnoid hemorrhage (aSAH).
Methods: In this prospective observational study, we quantified serum sSRA levels of 131 aSAH patients and 131 healthy controls. A poor outcome was defined as extended Glasgow outcome scale (GOSE) scores of 1-4 at 90 days after injury. Relations of serum sSRA levels to severity, delayed cerebral ischemia (DCI) and poor outcome were assessed using multivariate analysis. Predictive efficiency was determined via area under receiver operating characteristic curve (AUC).
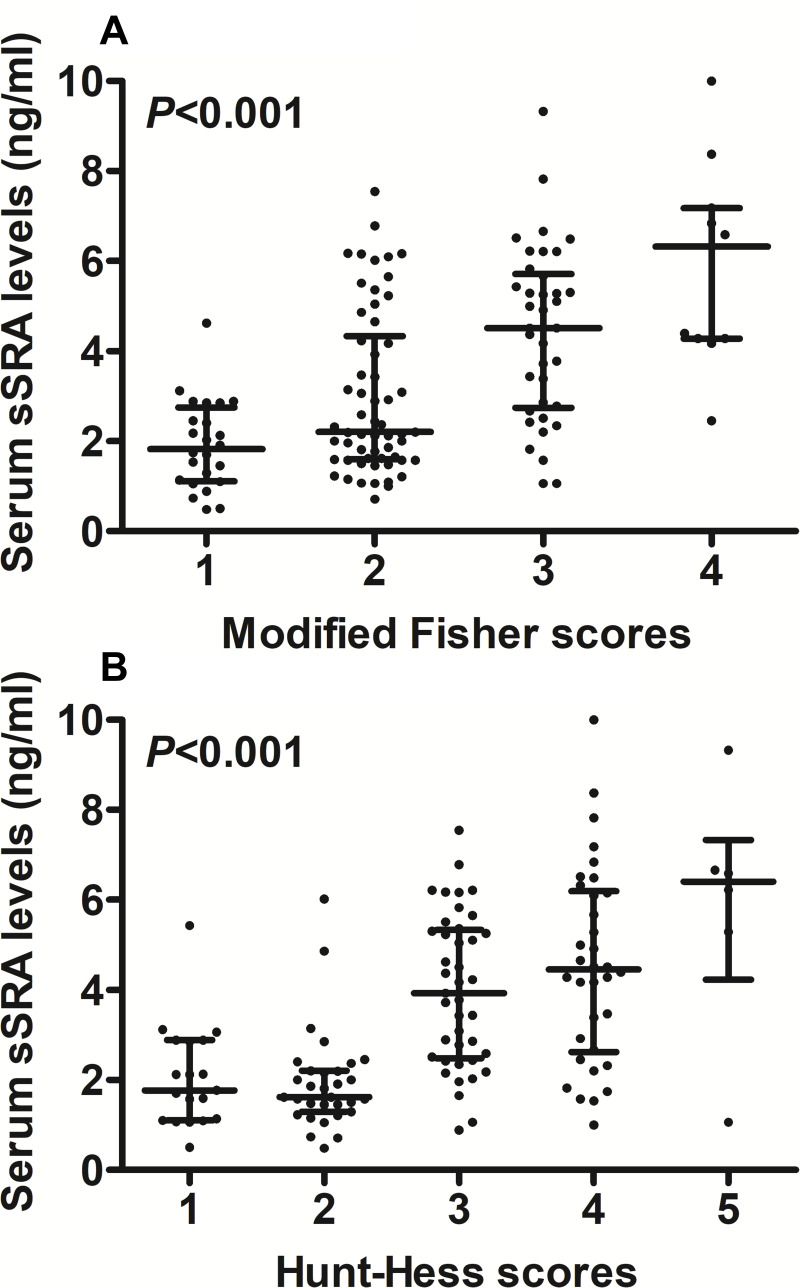
Results: Serum sSRA levels were markedly higher in aSAH patients than in controls (median, 2.9 ng/mL versus 1.0 ng/mL; P < 0.001). Serum sSRA levels were independently correlated with Hunt-Hess scores (beta, 0.569; 95% confidence interval (CI), 0.244-0.894; P = 0.001), modified Fisher scores (beta, 0.664; 95% CI, 0.254-1.074; P = 0.002) and 90-day GOSE scores (beta, -0.275; 95% CI, -0.440-0.110; P = 0.005). Serum sSRA levels independently predicted DCI (odds ratio, 1.305; 95% CI, 1.012-1.687; P = 0.040) and a poor outcome (odds ratio, 2.444; 95% CI, 1.264-4.726; P = 0.008), as well as showed significant accuracy for the discrimination of DCI (AUC, 0.753; 95% CI, 0.649-0.857; P < 0.001) and a poor outcome (AUC, 0.800; 95% CI, 0.721-0.880; P < 0.001). Its combination with Hunt-Hess scores and modified Fisher scores displayed significantly improved AUCs for predicting DCI and poor outcome, as compared to any of them (all P < 0.05).
Conclusion: There is a significant elevation of serum sSRA levels after aSAH, which in close correlation with illness severity, are independently associated with DCI and poor clinical outcome after aSAH. Hypothetically, SRA may regulate immune response in acute brain injury after aSAH and serum sSRA is presumed to be a potential prognostic biomarker of aSAH.
Keywords: aneurysm; biomarkers; delayed cerebral ischemia; mechanism; prognosis; scavenger receptor A; severity; subarachnoid hemorrhage.
© 2022 Jiang et al.
Conflict of interest statement
The authors report no conflicts of interest concerning the materials or methods used in this study or the findings specified in this article.
Figures





References
-
- Katsuki M, Kawamura S, Koh A. Easily created prediction model using automated artificial intelligence framework (Prediction One, Sony Network Communications Inc., Tokyo, Japan) for subarachnoid hemorrhage outcomes treated by coiling and delayed cerebral ischemia. Cureus. 2021;13(6):e15695. doi: 10.7759/cureus.15695 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
