

Acute outcomes for the full US cohort of the FLASH mechanical thrombectomy registry in pulmonary embolism
- PMID: 36349702
- PMCID: PMC9936254
- DOI: 10.4244/EIJ-D-22-00732
Acute outcomes for the full US cohort of the FLASH mechanical thrombectomy registry in pulmonary embolism
Abstract
Background: Evidence supporting interventional pulmonary embolism (PE) treatment is needed.
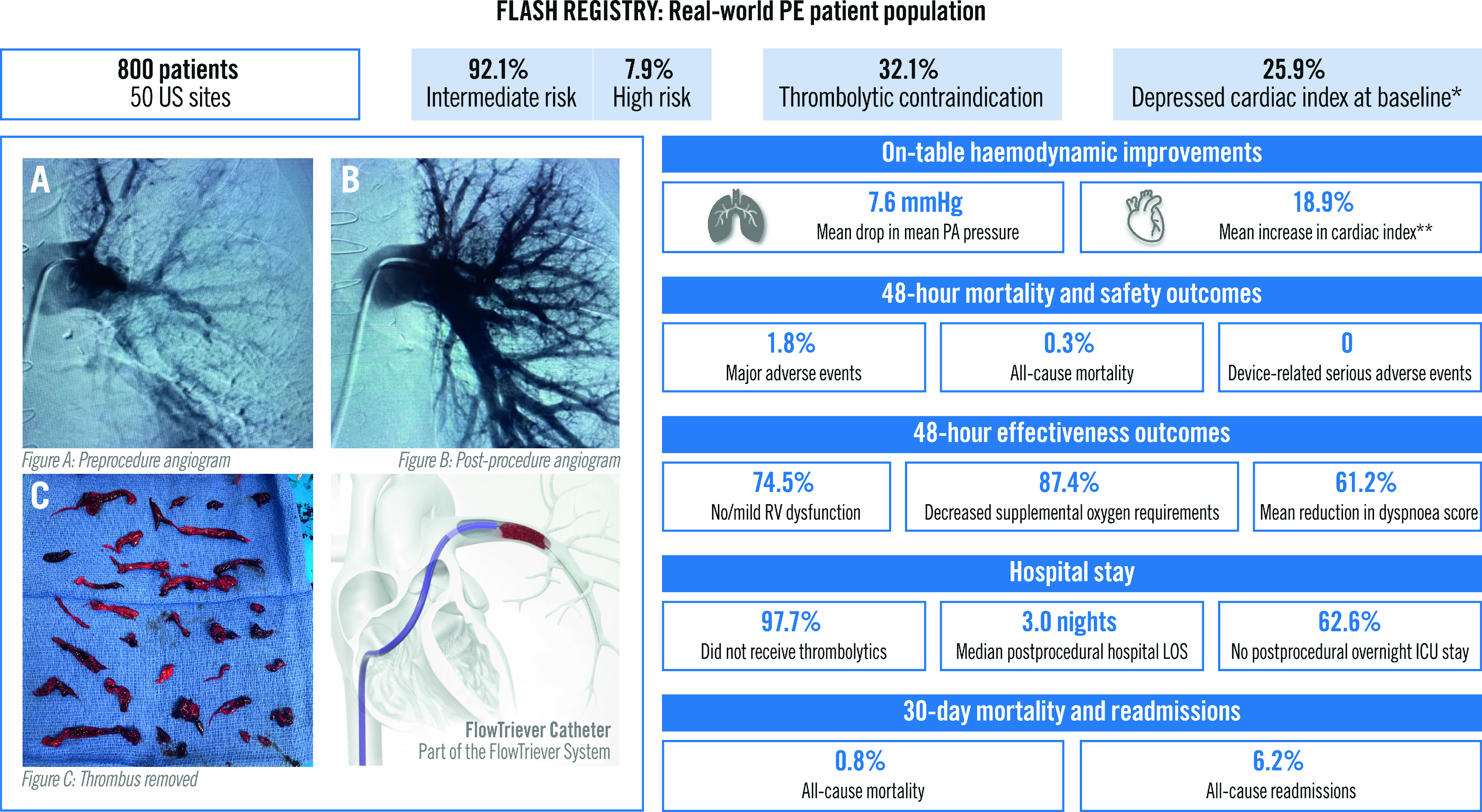
Aims: We aimed to evaluate the acute safety and effectiveness of mechanical thrombectomy for intermediate- and high-risk PE in a large real-world population.
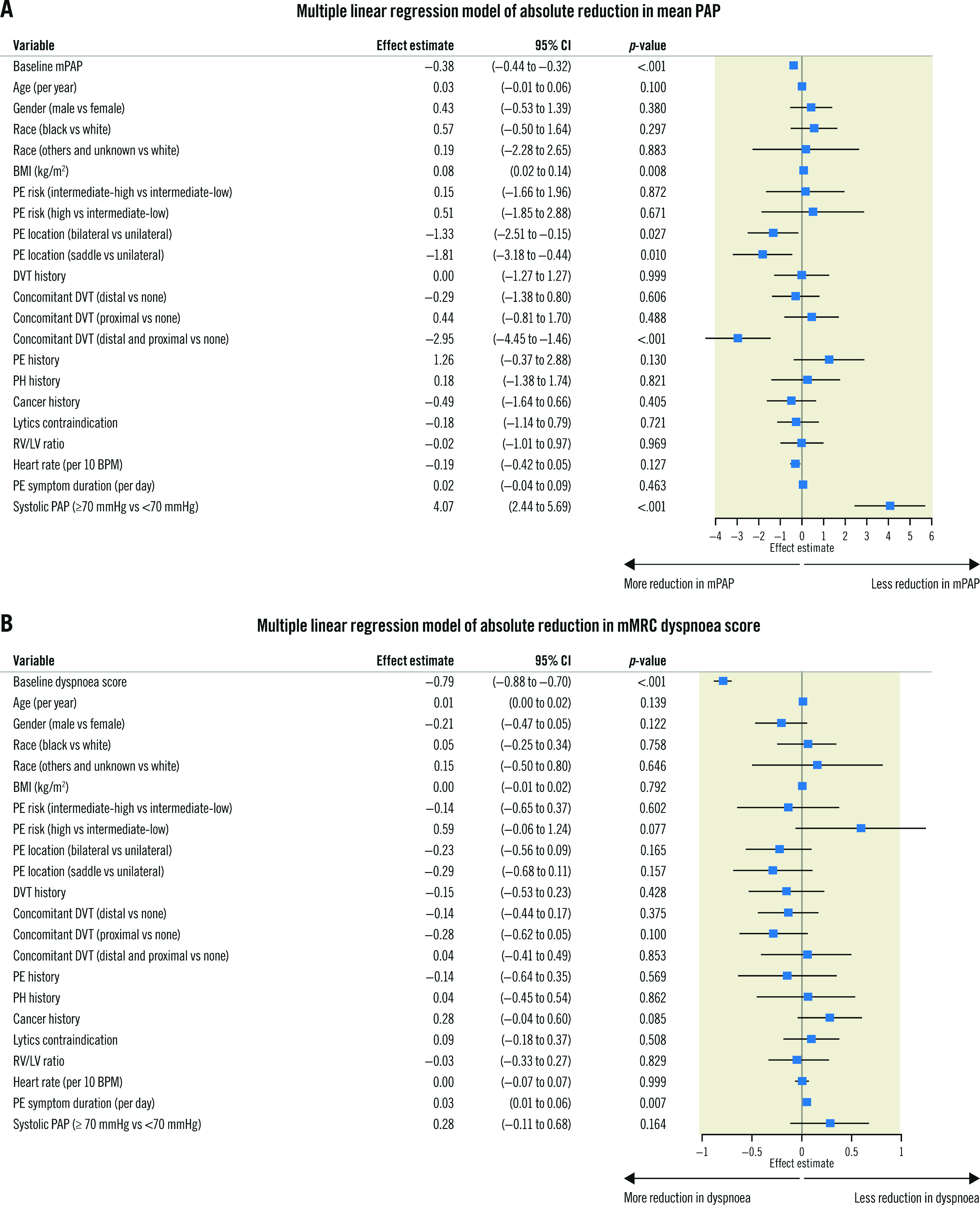
Methods: FLASH is a multicentre, prospective registry enrolling up to 1,000 US and European PE patients treated with mechanical thrombectomy using the FlowTriever System. The primary safety endpoint is a major adverse event composite including device-related death and major bleeding at 48 hours, and intraprocedural adverse events. Acute mortality and 48-hour outcomes are reported. Multivariate regression analysed characteristics associated with pulmonary artery pressure and dyspnoea improvement.
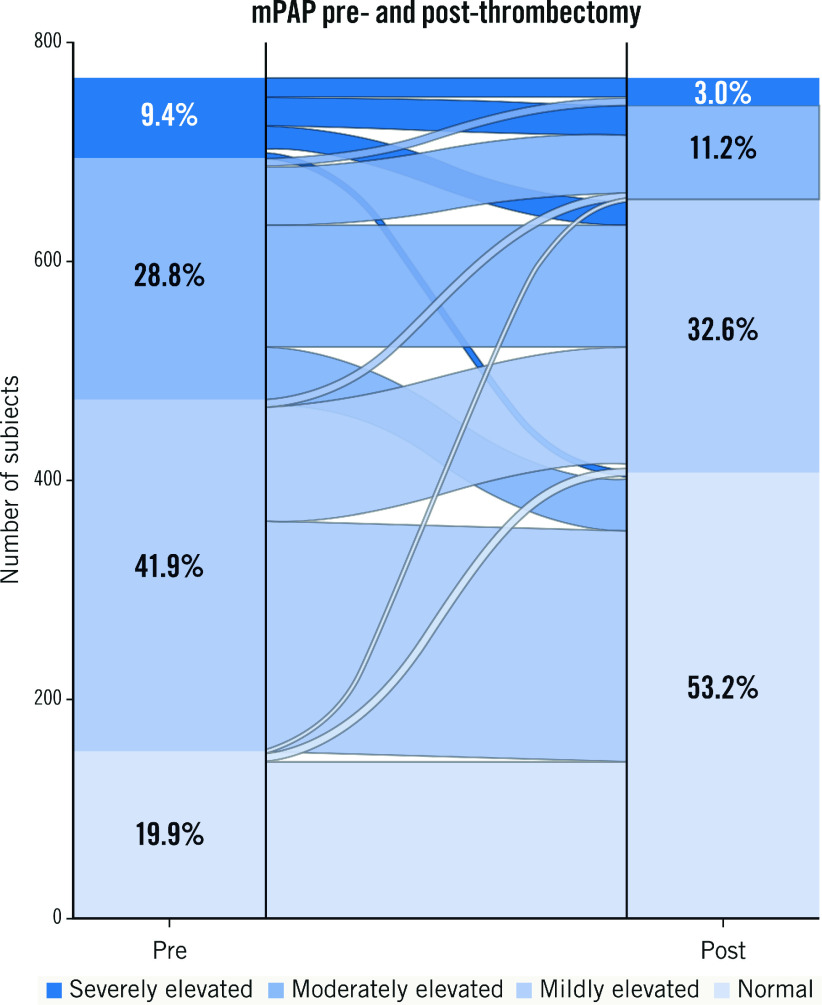
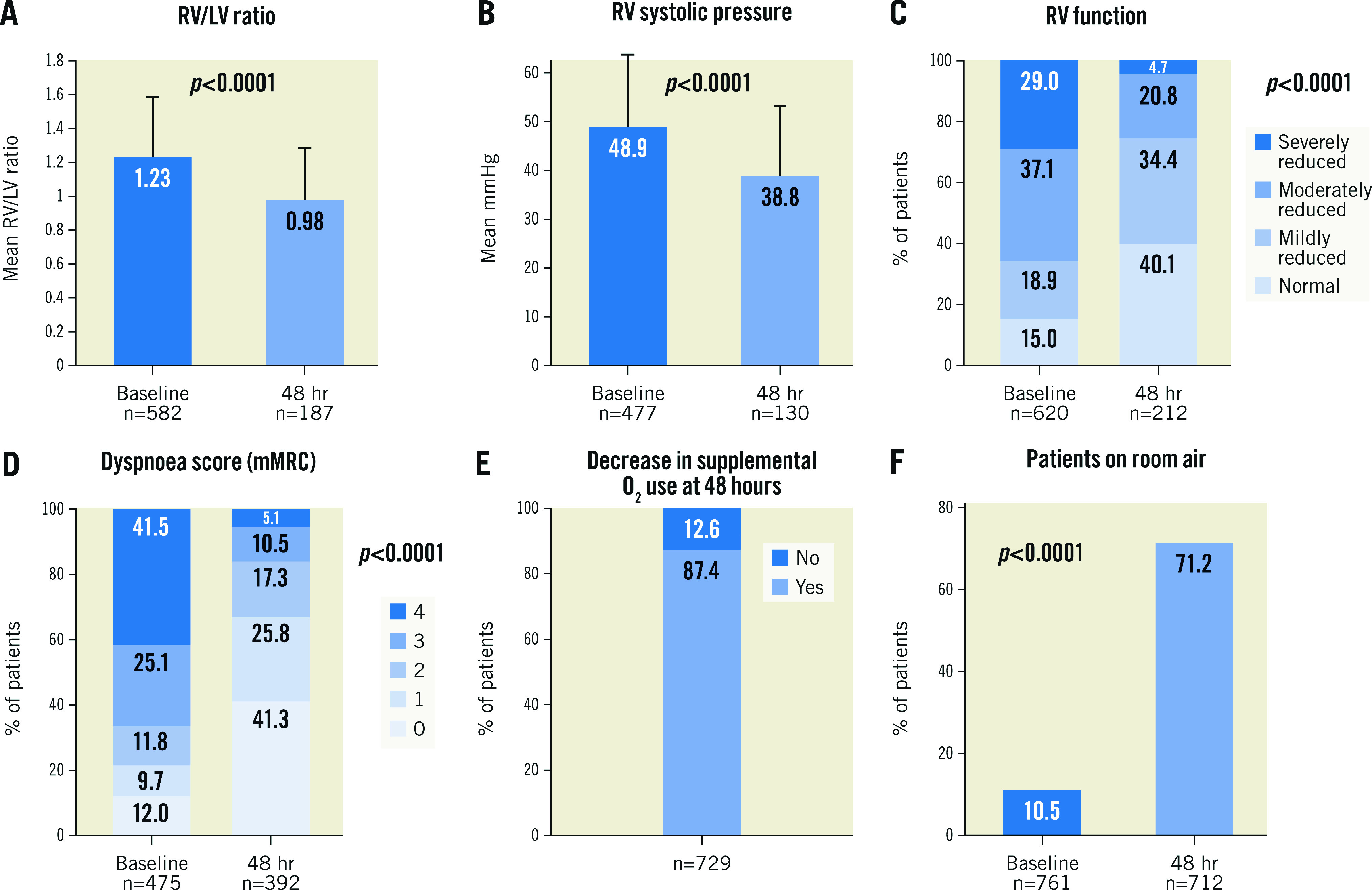
Results: Among 800 patients in the full US cohort, 76.7% had intermediate-high risk PE, 7.9% had high-risk PE, and 32.1% had thrombolytic contraindications. Major adverse events occurred in 1.8% of patients. All-cause mortality was 0.3% at 48-hour follow-up and 0.8% at 30-day follow-up, with no device-related deaths. Immediate haemodynamic improvements included a 7.6 mmHg mean drop in mean pulmonary artery pressure (-23.0%; p<0.0001) and a 0.3 L/min/m2 mean increase in cardiac index (18.9%; p<0.0001) in patients with depressed baseline values. Most patients (62.6%) had no overnight intensive care unit stay post-procedure. At 48 hours, the echocardiographic right ventricle/left ventricle ratio decreased from 1.23±0.36 to 0.98±0.31 (p<0.0001 for paired values) and patients with severe dyspnoea decreased from 66.5% to 15.6% (p<0.0001). Conclusions: Mechanical thrombectomy with the FlowTriever System demonstrates a favourable safety profile, improvements in haemodynamics and functional outcomes, and low 30-day mortality for intermediate- and high-risk PE.
Conflict of interest statement
C. Toma is a consultant to Medtronic and Philips. W.A. Jaber is a consultant to Inari Medical. M.D. Weinberg is a consultant to Boston Scientific, Magneto Thrombectomy Solutions, and Medtronic. M.C. Bunte receives institutional grant support from Inari Medical and is a consultant to Inari Medical, Abbott Labs, and Shockwave Medical. B. Stegman is a consultant to Edwards Lifesciences, Medtronic, Boston Scientific, and Forge Medical. R. Amin is a consultant to Inari Medical. H. Kado is a consultant to Inari Medical. M.A. Brown is a speaker for Inari Medical. M. Savin reports owning Inari Medical stock. J.M. Horowitz is a consultant to Inari Medical and Penumbra. The other authors have no conflicts of interest to declare.
Figures
References
-
- Sedhom R, Megaly M, Elbadawi A, Elgendy IY, Witzke CF, Kalra S, George JC, Omer M, Banerjee S, Jaber WA, Shishehbor MH. Contemporary National Trends and Outcomes of Pulmonary Embolism in the United States. Am J Cardiol. 2022;176:132–8. - PubMed
-
- Konstantinides SV, Meyer G, Becattini C, Bueno H, Geersing GJ, Harjola VP, Huisman MV, Humbert M, Jennings CS, Jiménez D, Kucher N, Lang IM, Lankeit M, Lorusso R, Mazzolai L, Meneveau N, Ní Áinle F, Prandoni P, Pruszczyk P, Righini M, Torbicki A, Belle V, Zamorano JL ESC Scientific Document Group. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur Heart J. 2020;41:543–603. - PubMed
-
- Meyer G, Vicaut E, Danays T, Agnelli G, Becattini C, Beyer-Westendorf J, Bluhmki E, Bouvaist H, Brenner B, Couturaud F, Dellas C, Empen K, Franca A, Galiè N, Geibel A, Goldhaber SZ, Jimenez D, Kozak M, Kupatt C, Kucher N, Lang IM, Lankeit M, Meneveau N, Pacouret G, Palazzini M, Petris A, Pruszczyk P, Rugolotto M, Salvi A, Schellong S, Sebbane M, Sobkowicz B, Stefanovic BS, Thiele H, Torbicki A, Verschuren F, Konstantinides SV PEITHO Investigators. Fibrinolysis for patients with intermediate-risk pulmonary embolism. N Engl J Med. 2014;370:1402–11. - PubMed
-
- Ismayl M, Machanahalli Balakrishna, Aboeata A, Gupta T, Young MN, Altin SE, Aronow HD, Goldsweig AM. Meta-Analysis Comparing Catheter-Directed Thrombolysis Versus Systemic Anticoagulation Alone for Submassive Pulmonary Embolism. Am J Cardiol. 2022;178:154–62. - PubMed
-
- Giri J, Sista AK, Weinberg I, Kearon C, Kumbhani DJ, Desai ND, Piazza G, Gladwin MT, Chatterjee S, Kobayashi T, Kabrhel C, Barnes GD. Interventional Therapies for Acute Pulmonary Embolism: Current Status and Principles for the Development of Novel Evidence: A Scientific Statement From the American Heart Association. Circulation. 2019;140:e774–801. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical