

Effects of melodic intonation therapy in patients with chronic nonfluent aphasia
- PMID: 36349876
- PMCID: PMC10262915
- DOI: 10.1111/nyas.14927
Effects of melodic intonation therapy in patients with chronic nonfluent aphasia
Abstract
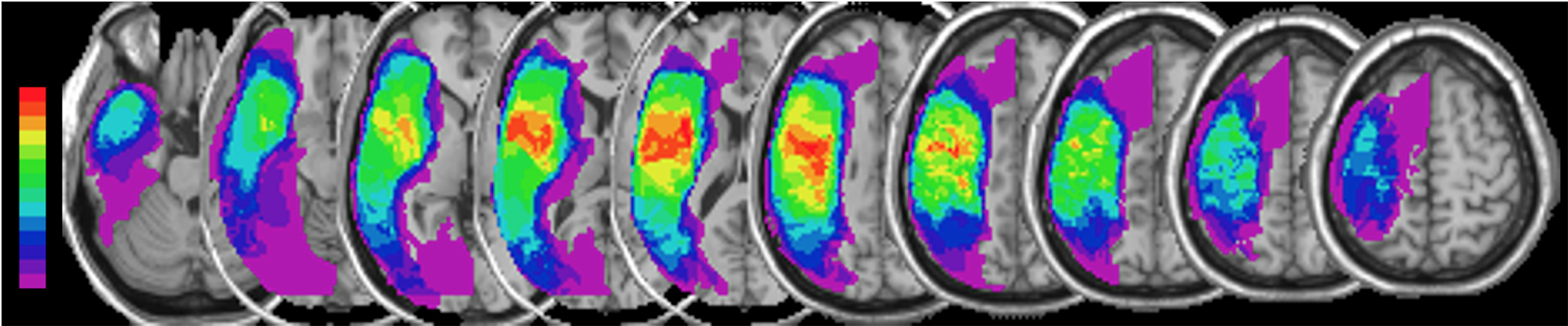
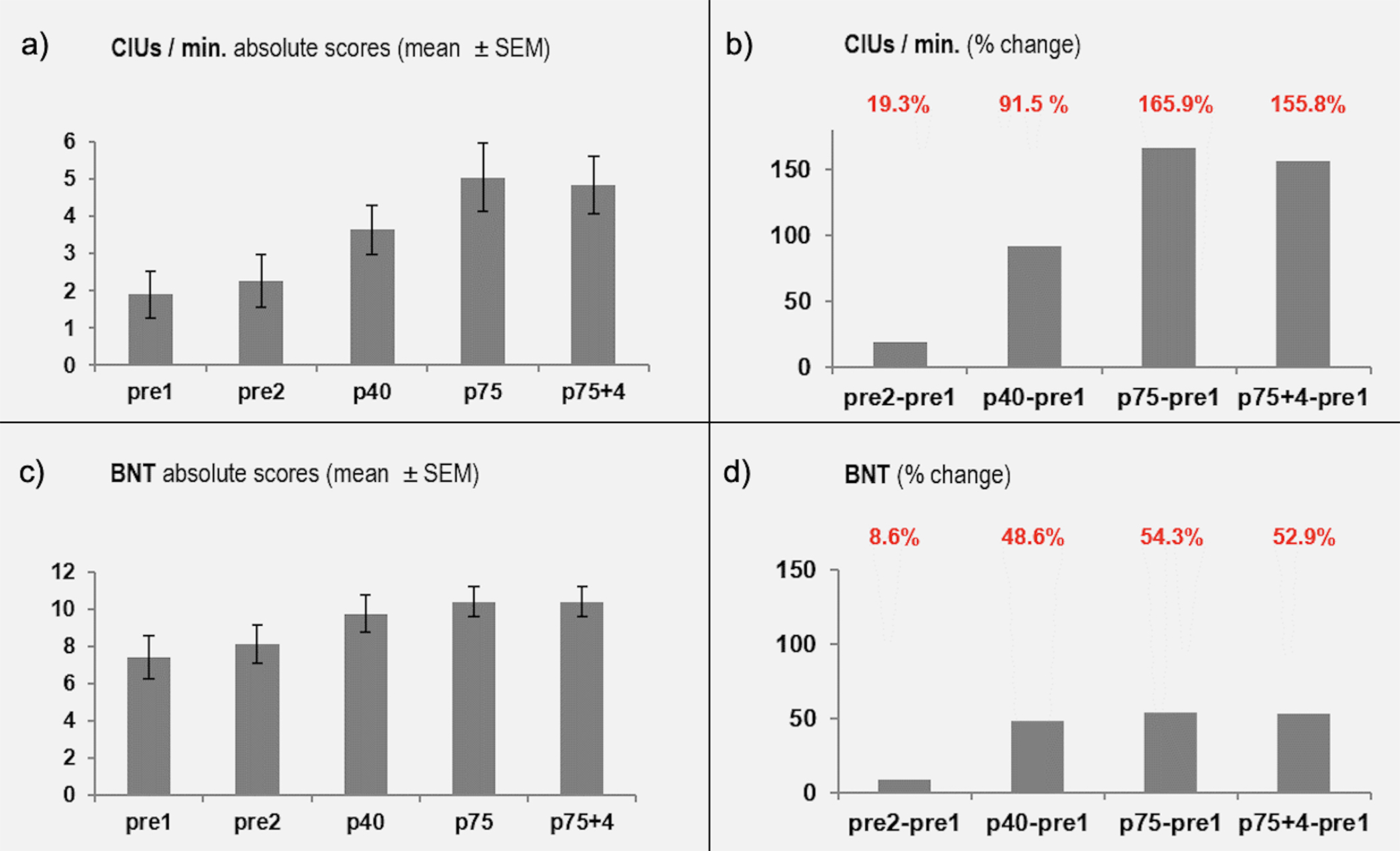
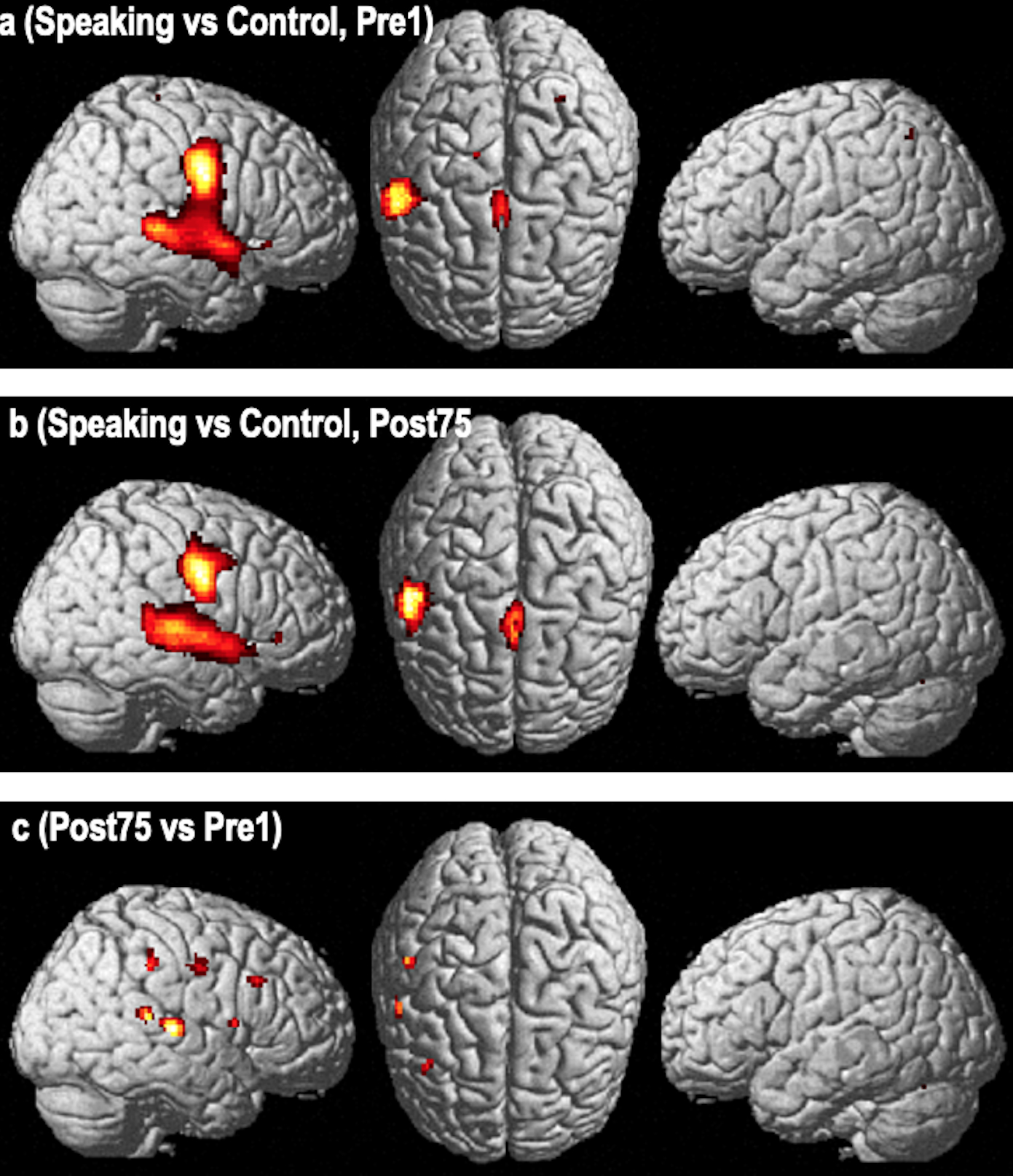
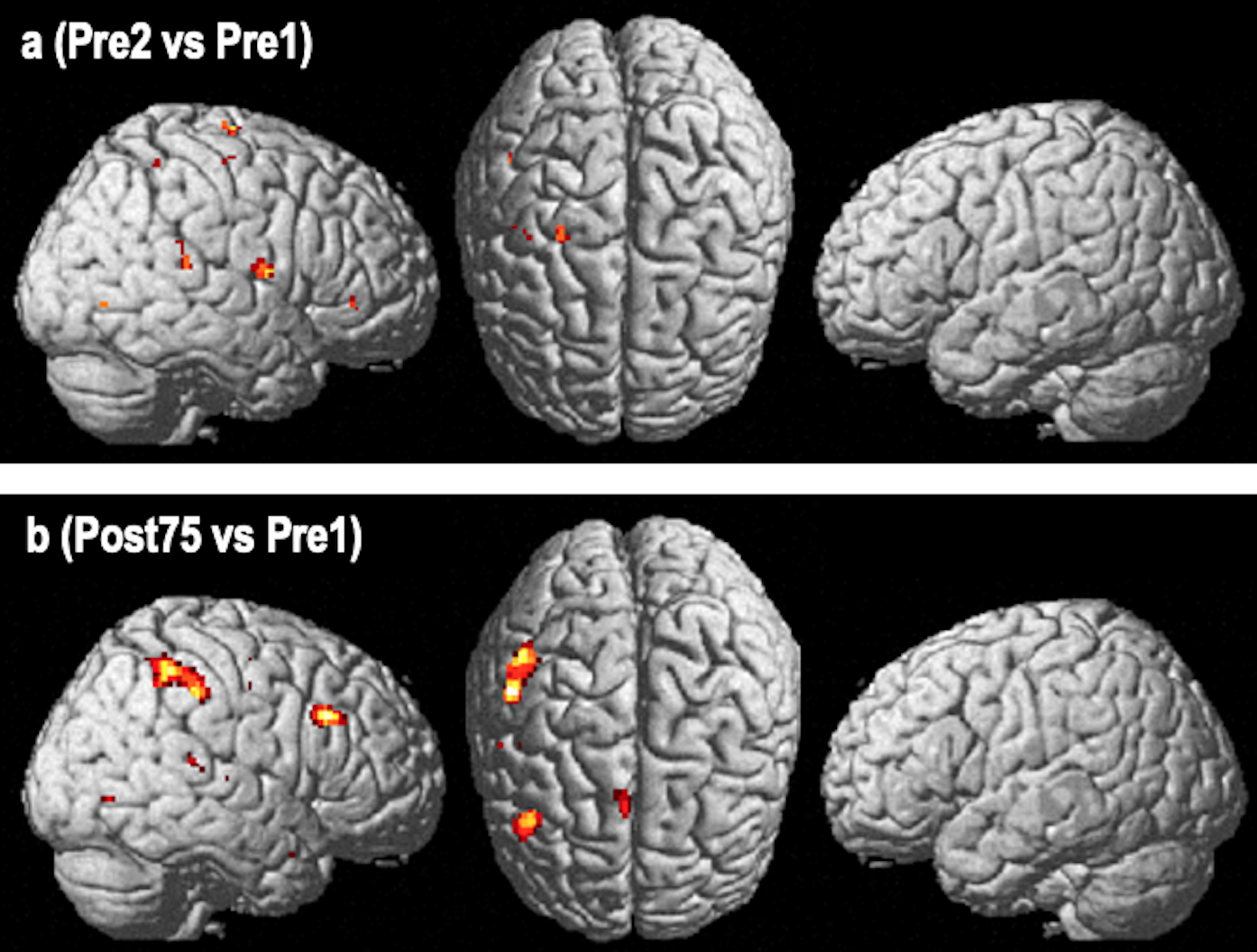
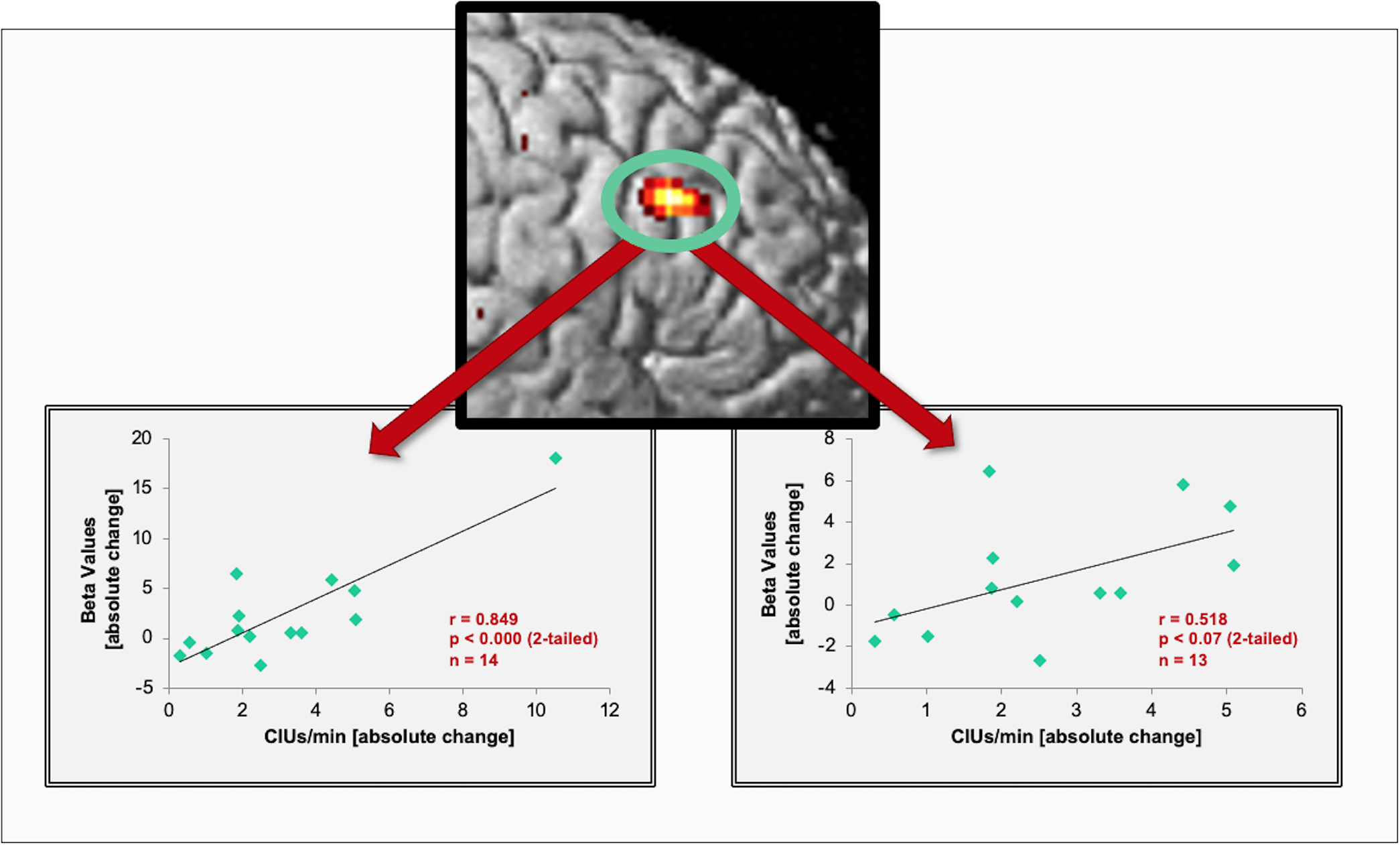
Patients with large left-hemisphere lesions and post-stroke aphasia often remain nonfluent. Melodic intonation therapy (MIT) may be an effective alternative to traditional speech therapy for facilitating recovery of fluency in those patients. In an open-label, proof-of-concept study, 14 subjects with nonfluent aphasia with large left-hemisphere lesions (171 ± 76 cc) underwent two speech/language assessments before, one at the midpoint, and two after the end of 75 sessions (1.5 h/session) of MIT. Functional MR imaging was done before and after therapy asking subjects to vocalize the same set of 10 bi-syllabic words. We found significant improvements in speech output after a period of intensive MIT (75 sessions for a total of 112.5 h) compared to two pre-therapy assessments. Therapy-induced gains were maintained 4 weeks post-treatment. Imaging changes were seen in a right-hemisphere network that included the posterior superior temporal and inferior frontal gyri, inferior pre- and postcentral gyri, pre-supplementary motor area, and supramarginal gyrus. Functional changes in the posterior right inferior frontal gyri significantly correlated with changes in a measure of fluency. Intense training of intonation-supported auditory-motor coupling and engaging feedforward/feedback control regions in the unaffected hemisphere improves speech-motor functions in subjects with nonfluent aphasia and large left-hemisphere lesions.
Keywords: MRI; aphasia; melodic intonation therapy; neuroplasticity; neurorehabilitation; stroke recovery.
© 2022 New York Academy of Sciences.
Conflict of interest statement
COMPETING INTERESTS
None
Figures
References
-
- Kertesz A, Harlock W, & Coates R (1979). Computer tomographic localization, lesion size, and prognosis in aphasia and nonverbal impairment. Brain Lang, 8(1), 34–50. - PubMed
-
- Pedersen PM, Vinter K, & Olsen TS (2004). Aphasia after stroke: type, severity and prognosis. The Copenhagen aphasia study. Cerebrovasc Dis, 17(1), 35–43. - PubMed
-
- Pedersen PM, Jorgensen HS, Nakayama H, Raaschou HO, & Olsen TS (1995). Aphasia in acute stroke: incidence, determinants, and recovery. Ann Neurol, 38, 659–666. - PubMed
-
- Rosen HJ, Petersen SE, Linenweber MR, Snyder AZ, White DA, Chapman L, Dromerick AW, Fiez JA, & Corbetta MD (2000). Neural correlates of recovery from aphasia after damage to left inferior frontal cortex. Neurology, 55(12), 1883–1894. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
