

Carotid atherosclerosis: An independent risk factor for small fiber nerve dysfunction in patients with type 2 diabetes mellitus
- PMID: 36350031
- PMCID: PMC9889662
- DOI: 10.1111/jdi.13936
Carotid atherosclerosis: An independent risk factor for small fiber nerve dysfunction in patients with type 2 diabetes mellitus
Abstract
Aims/introduction: To explore whether carotid atherosclerosis is an independent risk factor for small fiber nerve dysfunction in type 2 diabetes mellitus patients.
Materials and methods: A total of 247 type 2 diabetes patients from Nanjing Drum Tower Hospital received carotid ultrasonography and quantitative sensory testing, including cold and warm detection thresholds, and some patients received cold and heat pain detection thresholds, respectively. According to the results of quantitative sensory testing, patients were divided into normal small fiber nerve function (NSF) and small fiber nerve dysfunction (SFD) group. Meanwhile, patients were divided into the non-carotid atherosclerosis group, carotid intimal thickening, unilateral carotid atherosclerosis and bilateral carotid atherosclerosis group. The correlation between carotid ultrasonography with quantitative sensory testing parameters was analyzed by SPSS 26.0.
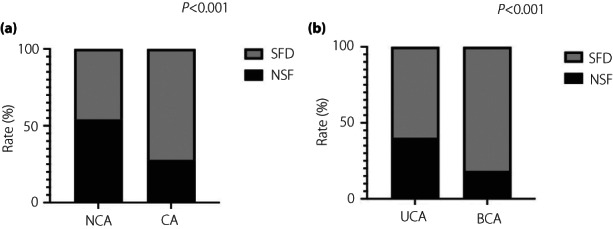
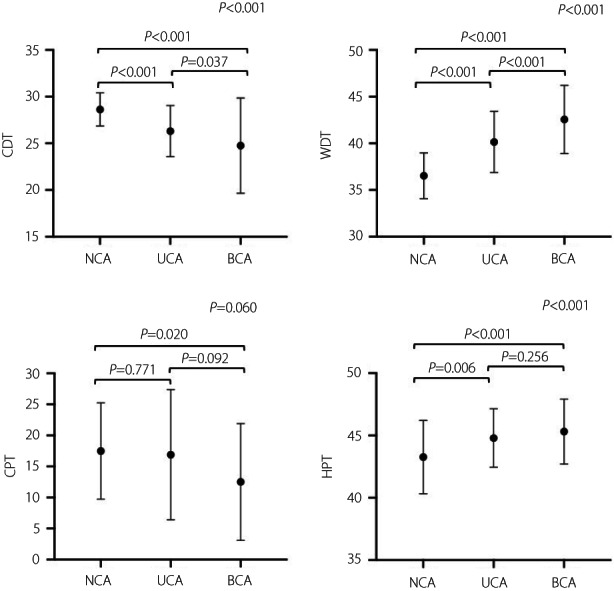
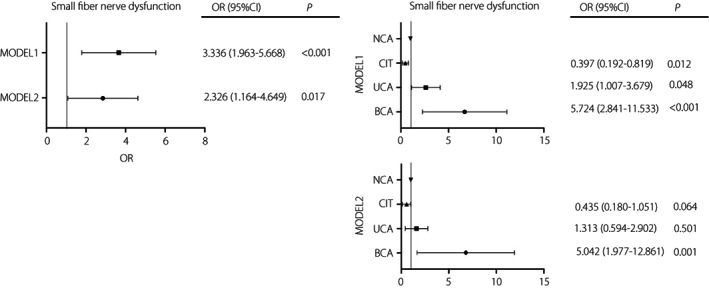
Results: First, the incidence rate of SFD increased significantly in patients with carotid atherosclerosis (72.2%, P < 0.001) especially in bilateral carotid atherosclerosis (81.7%, P < 0.001). Second, compared with the NS group, the carotid intima-media thickness in SFD was thicker (P = 0.018) and the size of atherosclerotic plaque was larger (P < 0.001). In addition, the cold detection threshold decreased (P < 0.001), whereas the warm detection threshold (P < 0.001) and heat pain detection threshold (P < 0.001) increased as aggravation of carotid atherosclerosis. In the correlation analysis, the size of atherosclerotic plaque presented a positive correlation with the warm detection threshold (r = 0.476, P < 0.001) and heat pain detection threshold (r = 0.213, P < 0.001), but presented a negative correlation with the cold detection threshold (r = -0.239, P < 0.01). Furthermore, carotid atherosclerosis (odds ratio 2.326, P = 0.017), especially bilateral carotid atherosclerosis (odds ratio 5.042, P = 0.001), was an independent risk factor for SFD (P < 0.05).
Conclusions: Carotid atherosclerosis was significantly associated with quantitative sensory testing and found to be an independent risk factor for small fiber nerve dysfunction in type 2 diabetes patients.
Keywords: Carotid atherosclerosis; Quantitative sensory testing; Small fiber neuropathy; Type 2 diabetes mellitus.
© 2022 The Authors. Journal of Diabetes Investigation published by Asian Association for the Study of Diabetes (AASD) and John Wiley & Sons Australia, Ltd.
Figures
Similar articles
-
Quantitative sensory testing can effectively predict cardiovascular autonomic neuropathy in patients with type 2 diabetes mellitus.Acta Diabetol. 2021 Nov;58(11):1541-1549. doi: 10.1007/s00592-021-01744-4. Epub 2021 Jun 17. Acta Diabetol. 2021. PMID: 34137938
-
Low-normal serum unconjugated bilirubin levels are associated with late but not early carotid atherosclerotic lesions in T2DM subjects.Front Endocrinol (Lausanne). 2022 Nov 2;13:948338. doi: 10.3389/fendo.2022.948338. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 36407305 Free PMC article.
-
Genetic determinants of blood pressure traits are associated with carotid arterial thickening and plaque formation in patients with type 2 diabetes.Diab Vasc Dis Res. 2019 Jan;16(1):13-21. doi: 10.1177/1479164118810365. Diab Vasc Dis Res. 2019. PMID: 30789093
-
Altered pain processing in patients with type 1 and 2 diabetes: systematic review and meta-analysis of pain detection thresholds and pain modulation mechanisms.BMJ Open Diabetes Res Care. 2020 Aug;8(1):e001566. doi: 10.1136/bmjdrc-2020-001566. BMJ Open Diabetes Res Care. 2020. PMID: 32868312 Free PMC article.
-
Relationship of Neutrophil-to-Lymphocyte Ratio with Carotid Plaque Vulnerability and Occurrence of Vulnerable Carotid Plaque in Patients with Acute Ischemic Stroke.Biomed Res Int. 2021 Jun 21;2021:6894623. doi: 10.1155/2021/6894623. eCollection 2021. Biomed Res Int. 2021. PMID: 34250090 Free PMC article. Review.
Cited by
-
Interpretable machine learning models for detecting peripheral neuropathy and lower extremity arterial disease in diabetics: an analysis of critical shared and unique risk factors.BMC Med Inform Decis Mak. 2024 Jul 22;24(1):200. doi: 10.1186/s12911-024-02595-z. BMC Med Inform Decis Mak. 2024. PMID: 39039521 Free PMC article.
References
-
- Uusitupa M, Siitonen O, Aro A, et al. Prevalence of coronary heart disease, left ventricular failure and hypertension in middle‐aged, newly diagnosed type 2 (non‐insulin‐dependent) diabetic subjects. Diabetologia 1985; 28: 22–27. - PubMed
-
- Devigili G, Cazzato D, Lauria G. Clinical diagnosis and management of small fiber neuropathy: An update on best practice. Expert Rev Neurother 2020; 20: 967–980. - PubMed
-
- Chan Amanda CY, Wilder‐Smith EP. Small fiber neuropathy: Getting bigger! Muscle Nerve 2016; 53: 671–682. - PubMed
-
- Itani M, Gylfadottir SS, Krøigård T, et al. Small and large fiber sensory polyneuropathy in type 2 diabetes: Influence of diagnostic criteria on neuropathy subtypes. J Peripher Nerv Syst 2021; 26: 55–65. - PubMed
-
- Kurokawa R, Murata H, Ogino M, et al. Altered blood flow distribution in the rat spinal cord under chronic compression. Spine (Phila Pa 1976) 2011; 36: 1006–1009. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
