

Model-informed precision dosing of beta-lactam antibiotics and ciprofloxacin in critically ill patients: a multicentre randomised clinical trial
- PMID: 36350354
- PMCID: PMC9645317
- DOI: 10.1007/s00134-022-06921-9
Model-informed precision dosing of beta-lactam antibiotics and ciprofloxacin in critically ill patients: a multicentre randomised clinical trial
Abstract
Purpose: Individualising drug dosing using model-informed precision dosing (MIPD) of beta-lactam antibiotics and ciprofloxacin has been proposed as an alternative to standard dosing to optimise antibiotic efficacy in critically ill patients. However, randomised clinical trials (RCT) on clinical outcomes have been lacking.
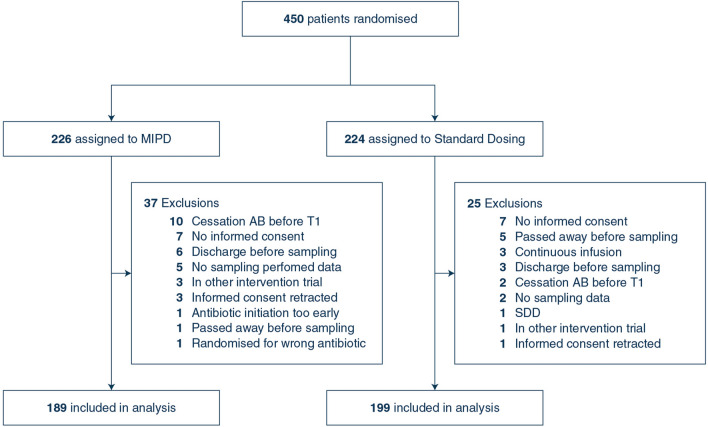
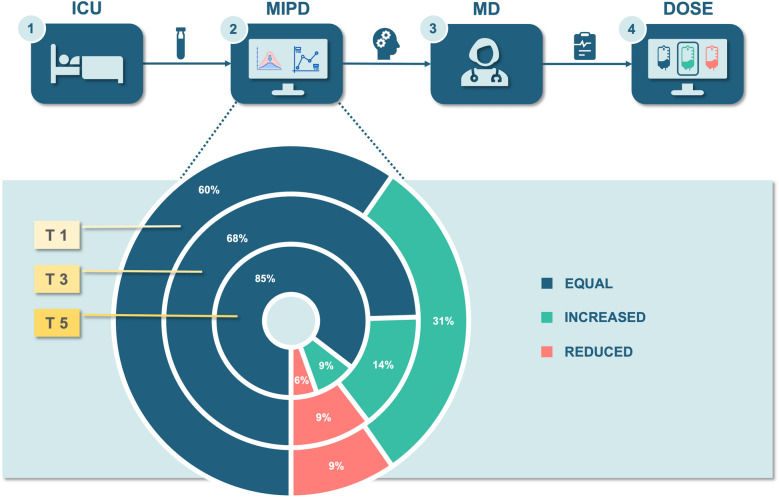
Methods: This multicentre RCT, including patients admitted to the intensive care unit (ICU) who were treated with antibiotics, was conducted in eight hospitals in the Netherlands. Patients were randomised to MIPD with dose and interval adjustments based on monitoring serum drug levels (therapeutic drug monitoring) combined with pharmacometric modelling of beta-lactam antibiotics and ciprofloxacin. The primary outcome was ICU length of stay (LOS). Secondary outcomes were ICU mortality, hospital mortality, 28-day mortality, 6-month mortality, delta sequential organ failure assessment (SOFA) score, adverse events and target attainment.
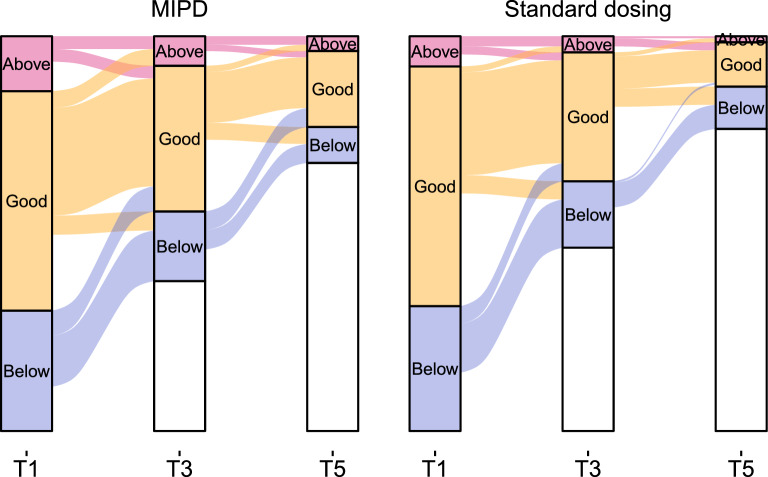
Results: In total, 388 (MIPD n = 189; standard dosing n = 199) patients were analysed (median age 64 [IQR 55-71]). We found no significant differences in ICU LOS between MIPD compared to standard dosing (10 MIPD vs 8 standard dosing; IRR = 1.16; 95% CI 0.96-1.41; p = 0.13). There was no significant difference in target attainment before intervention at day 1 (T1) (55.6% MIPD vs 60.9% standard dosing; p = 0.24) or at day 3 (T3) (59.5% vs 60.4%; p = 0.84). There were no significant differences in other secondary outcomes.
Conclusions: We could not show a beneficial effect of MIPD of beta-lactam antibiotics and ciprofloxacin on ICU LOS in critically ill patients. Our data highlight the need to identify other approaches to dose optimisation.
Keywords: Beta-lactam antibiotics; Ciprofloxacin; Critically ill; Model-informed; Precision dosing.
© 2022. The Author(s).
Conflict of interest statement
All authors reported no possible competing interests.
Figures
Comment in
-
Advancing precision-based antimicrobial dosing in critically ill patients.Intensive Care Med. 2023 Mar;49(3):324-326. doi: 10.1007/s00134-022-06969-7. Epub 2023 Jan 25. Intensive Care Med. 2023. PMID: 36695835 No abstract available.
References
-
- Bassetti M, Rello J, Blasi F, Goossens H, Sotgiu G, Tavoschi L, Zasowski EJ, Arber MR, McCool R, Patterson JV, Longshaw CM, Lopes S, Manissero D, Nguyen ST, Tone K, Aliberti S. Systematic review of the impact of appropriate versus inappropriate initial antibiotic therapy on outcomes of patients with severe bacterial infections. Int J Antimicrob Agents. 2020;56:106184. doi: 10.1016/j.ijantimicag.2020.106184. - DOI - PubMed
-
- Axente C, Licker M, Moldovan R, Hogea E, Muntean D, Horhat F, Bedreag O, Sandesc D, Papurica M, Dugaesescu D, Voicu M, Baditoiu L. Antimicrobial consumption, costs and resistance patterns: a two year prospective study in a Romanian intensive care unit. BMC Infect Dis. 2017;17:358. doi: 10.1186/s12879-017-2440-7. - DOI - PMC - PubMed
-
- Dulhunty JM, Webb SAR, Paterson DL, Bellomo R, Myburgh J, Roberts JA, Lipman J. A survey of antibiotic prescribing practices in Australian and New Zealand intensive care units. Crit Care Resusc. 2010;12:162–170. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
