

Delivery of Lung-protective Ventilation for Acute Respiratory Distress Syndrome: A Hybrid Implementation-Effectiveness Trial
- PMID: 36350983
- PMCID: PMC9993149
- DOI: 10.1513/AnnalsATS.202207-626OC
Delivery of Lung-protective Ventilation for Acute Respiratory Distress Syndrome: A Hybrid Implementation-Effectiveness Trial
Abstract
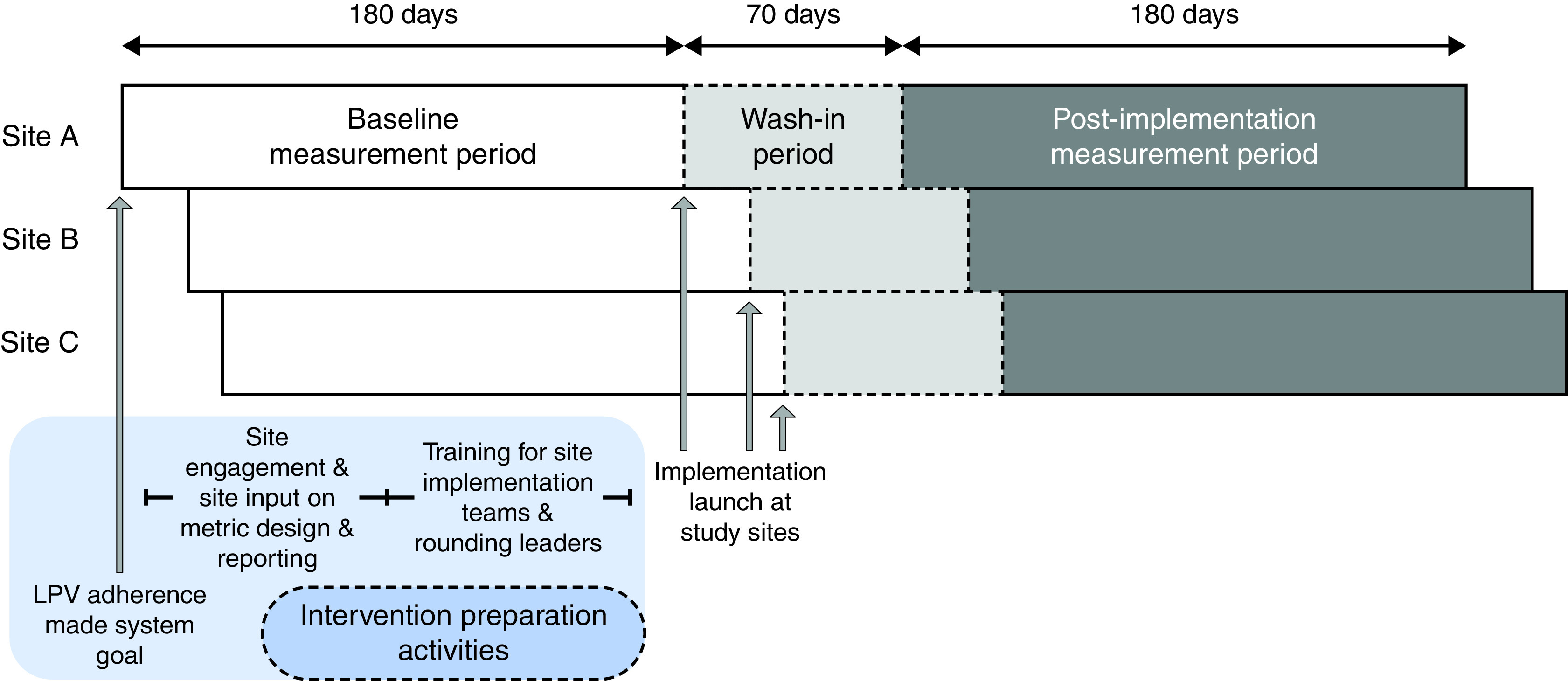
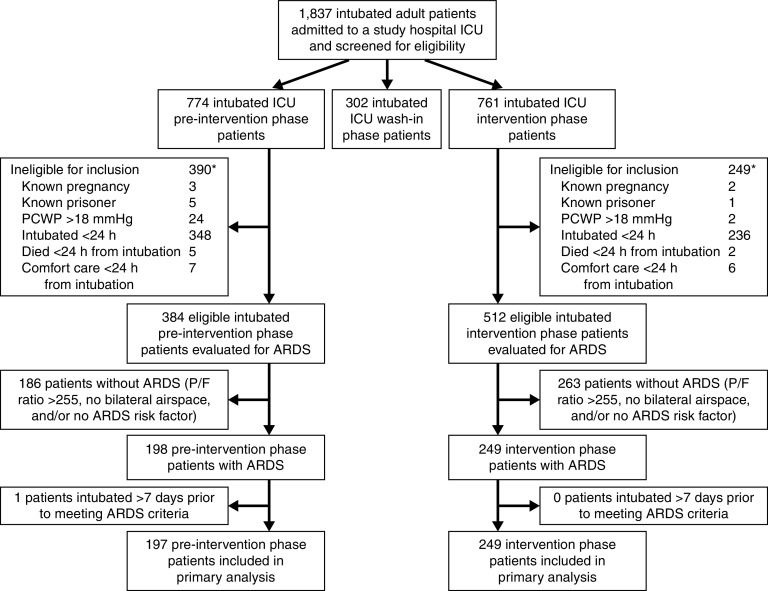
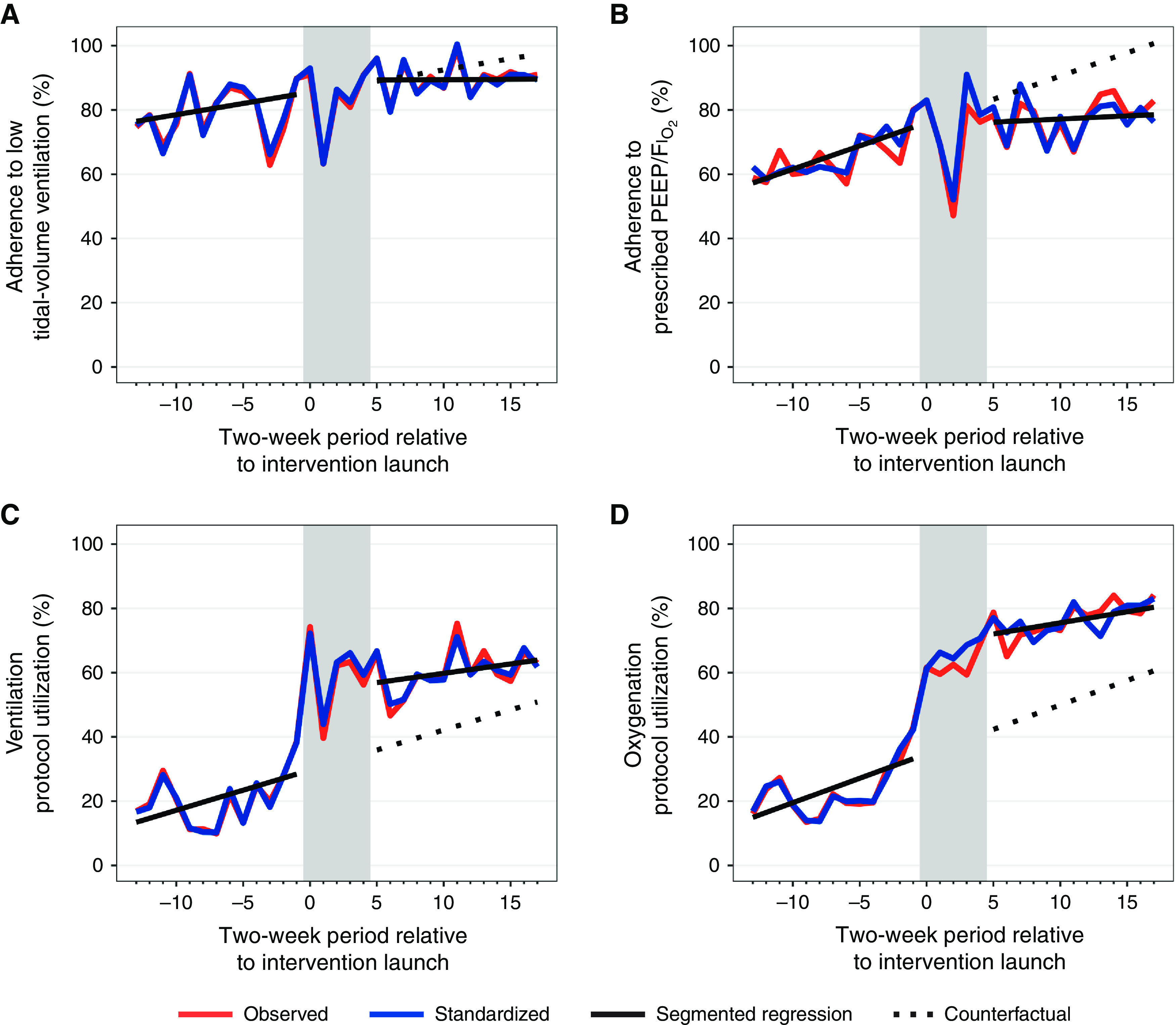
Rationale: Lung-protective ventilation (LPV) improves outcomes for patients with acute respiratory distress syndrome (ARDS), but adherence remains inadequate. Objectives: To measure the process and clinical impacts of implementation of a science-based intervention to improve LPV adherence for patients with ARDS, in part by increased use of clinical decision support (CDS). Methods: We conducted a type III hybrid implementation/effectiveness pilot trial enrolling adult patients with ARDS admitted to three hospitals before and after the launch of a multimodal implementation intervention to increase the use of mechanical ventilation CDS and improve LPV adherence. The primary outcome was patients' percentage of time adherent to low tidal volume (⩽6.5 ml/kg predicted body weight) ventilation (LTVV). Secondary outcomes included adherence to prescribed oxygenation settings, the use of the CDS tool's independent oxygenation and ventilation components, ventilator-free days, and mortality. Analyses employed multivariable regression to compare adjusted pre- versus postintervention outcomes after the exclusion of a postintervention wash-in period. A sensitivity analysis measured process outcomes' level and trend change postintervention using segmented regression. Results: The 446 included patients had a mean age of 60 years, and 43% were female. Demographic and clinical characteristics were similar pre- versus postintervention. The adjusted proportion of adherent time increased postintervention for LTVV (9.2%; 95% confidence interval [CI], 3.8-14.5%) and prescribed oxygenation settings (11.9%; 95% CI, 7.2-16.5%), as did the probability patients spent ⩾90% of ventilated time on LTVV (adjusted odds ratio [aOR] 2.58; 95% CI, 1.64-4.10) and use of ventilation CDS (aOR, 41.3%; 95% CI, 35.9-46.7%) and oxygenation CDS (aOR, 54.3%; 95% CI, 50.9-57.7%). Ventilator-free days (aOR, 1.15; 95% CI, 0.81-1.62) and 28-day mortality (aOR, 0.78; 95% CI, 0.50-1.20) did not change significantly after intervention. Segmented regression analysis supported a causal relationship between the intervention and improved CDS usage but suggested trends before intervention rather than the studied intervention could explain increased LPV adherence after the intervention. Conclusions: In this pilot trial, a multimodal implementation intervention was associated with increased use of ventilator management CDS for patients with ARDS but was not associated with differences in clinical outcomes and may not have independently caused the observed postintervention improvements in LPV adherence. Clinical trial registered with www.clinicaltrials.gov (NCT03984175).
Keywords: acute respiratory distress syndrome; clinical decision support; implementation science; invasive mechanical ventilation; low tidal volume ventilation.
Figures
Comment in
-
Shortening the Journey from Evidence to Practice: The Benefits and Complexities of Hybrid Implementation-effectiveness Trials.Ann Am Thorac Soc. 2023 Mar;20(3):366-368. doi: 10.1513/AnnalsATS.202211-972ED. Ann Am Thorac Soc. 2023. PMID: 36856716 Free PMC article. No abstract available.
References
-
- Bellani G, Laffey JG, Pham T, Fan E, Brochard L, Esteban A, et al. LUNG SAFE Investigators ESICM Trials Group. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA . 2016;315:788–800. - PubMed
-
- Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E, et al. ARDS Definition Task Force Acute respiratory distress syndrome: the Berlin definition. JAMA . 2012;307:2526–2533. - PubMed
-
- Lanspa MJ, Gong MN, Schoenfeld DA, Lee KT, Grissom CK, Hou PC, et al. The National Heart, Lung, and Blood Institute Prevention and Early Treatment of Acute Lung Injury (PETAL) Clinical Trials Network Prospective assessment of the feasibility of a trial of low-tidal volume ventilation for patients with acute respiratory failure. Ann Am Thorac Soc . 2019;16:356–362. - PMC - PubMed
-
- Brower RG, Matthay MA, Morris A, Schoenfeld D, Thompson BT, Wheeler A, Acute Respiratory Distress Syndrome Network Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med . 2000;342:1301–1308. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
