

Pregnancy induces pancreatic insulin secretion in women with long-standing type 1 diabetes
- PMID: 36351678
- PMCID: PMC9644305
- DOI: 10.1136/bmjdrc-2022-002948
Pregnancy induces pancreatic insulin secretion in women with long-standing type 1 diabetes
Abstract
Introduction: Pregnancy entails both pancreatic adaptations with increasing β-cell mass and immunological alterations in healthy women. In this study, we have examined the effects of pregnancy on β-cell function and immunological processes in long-standing type 1 diabetes (L-T1D).
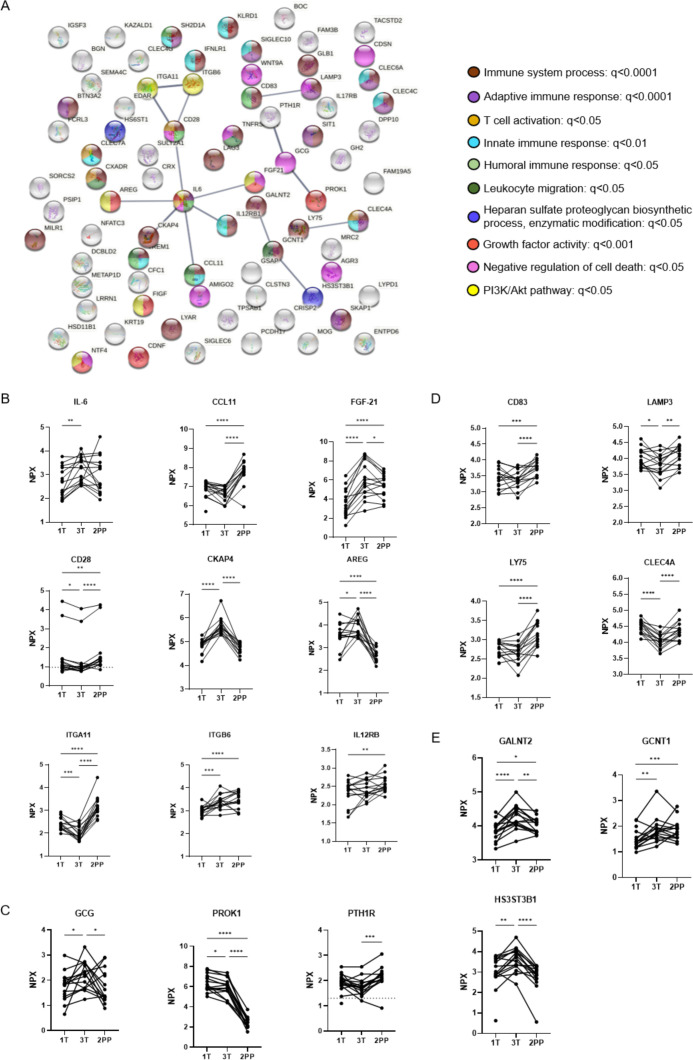
Research design and methods: Fasting and stimulated C-peptide were measured after an oral glucose tolerance test in pregnant women with L-T1D (n=17) during the first trimester, third trimester, and 5-8 weeks post partum. Two 92-plex Olink panels were used to measure proteins in plasma. Non-pregnant women with L-T1D (n=30) were included for comparison.
Results: Fasting C-peptide was detected to a higher degree in women with L-T1D during gestation and after parturition (first trimester: 64.7%, third trimester: 76.5%, and post partum: 64.7% vs 26.7% in non-pregnant women). Also, total insulin secretion and peak C-peptide increased during pregnancy. The plasma protein levels in pregnant women with L-T1D was dynamic, but few analytes were functionally related. Specifically, peripheral levels of prolactin (PRL), prokineticin (PROK)-1, and glucagon (GCG) were elevated during gestation whereas levels of proteins related to leukocyte migration (CCL11), T cell activation (CD28), and antigen presentation (such as CD83) were reduced.
Conclusions: In summary, we have found that some C-peptide secretion, that is, an indirect measurement of endogenous insulin production, is regained in women with L-T1D during pregnancy, which might be attributed to elevated peripheral levels of PRL, PROK-1, or GCG.
Keywords: C-peptide; diabetes mellitus, type 1; immunomodulation; pregnancy.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical