

Comparing walking with knee-ankle-foot orthoses and a knee-powered exoskeleton after spinal cord injury: a randomized, crossover clinical trial
- PMID: 36351989
- PMCID: PMC9646697
- DOI: 10.1038/s41598-022-23556-4
Comparing walking with knee-ankle-foot orthoses and a knee-powered exoskeleton after spinal cord injury: a randomized, crossover clinical trial
Abstract
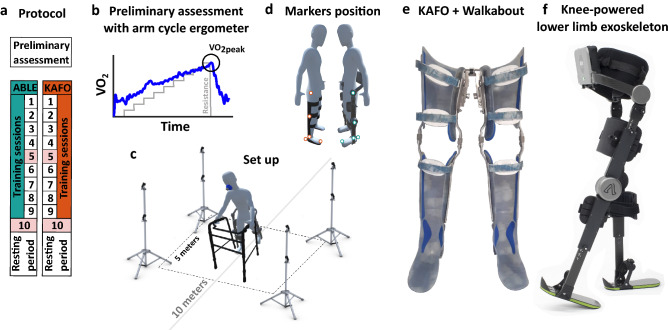
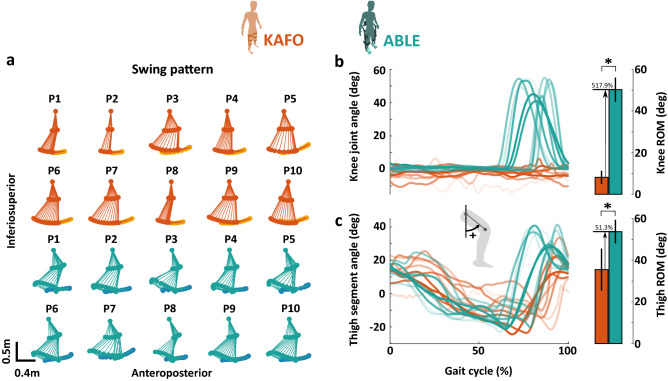
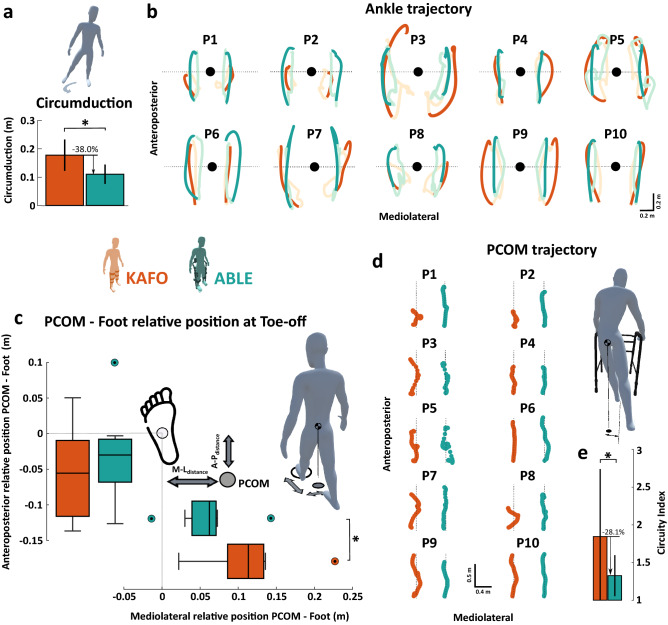
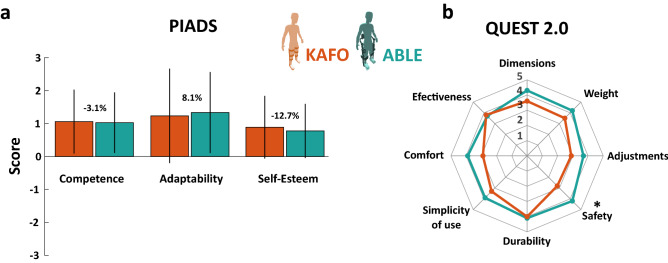
Recovering the ability to stand and walk independently can have numerous health benefits for people with spinal cord injury (SCI). Wearable exoskeletons are being considered as a promising alternative to conventional knee-ankle-foot orthoses (KAFOs) for gait training and assisting functional mobility. However, comparisons between these two types of devices in terms of gait biomechanics and energetics have been limited. Through a randomized, crossover clinical trial, this study compared the use of a knee-powered lower limb exoskeleton (the ABLE Exoskeleton) against passive orthoses, which are the current standard of care for verticalization and gait ambulation outside the clinical setting in people with SCI. Ten patients with SCI completed a 10-session gait training program with each device followed by user satisfaction questionnaires. Walking with the ABLE Exoskeleton improved gait kinematics compared to the KAFOs, providing a more physiological gait pattern with less compensatory movements (38% reduction of circumduction, 25% increase of step length, 29% improvement in weight shifting). However, participants did not exhibit significantly better results in walking performance for the standard clinical tests (Timed Up and Go, 10-m Walk Test, and 6-min Walk Test), nor significant reductions in energy consumption. These results suggest that providing powered assistance only on the knee joints is not enough to significantly reduce the energy consumption required by people with SCI to walk compared to passive orthoses. Active assistance on the hip or ankle joints seems necessary to achieve this outcome.
© 2022. The Author(s).
Conflict of interest statement
J.L-P. is an employee and receives salary from ABLE Human Motion S.L. (Barcelona, Spain), which was the sponsor of the present clinical investigation and manufacturer of the ABLE Exoskeleton. J.M.F-L. is co-founder and owns stock in the company ABLE Human Motion S.L. (Barcelona, Spain), which was the sponsor of the present clinical investigation and manufacturer of the ABLE Exoskeleton. The other authors declare no competing interests.
Figures


References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
