

Monitoring and management of chronic kidney disease in ambulatory care - analysis of clinical and claims data from a population-based study
- PMID: 36352433
- PMCID: PMC9644486
- DOI: 10.1186/s12913-022-08691-y
Monitoring and management of chronic kidney disease in ambulatory care - analysis of clinical and claims data from a population-based study
Abstract
Background: Although chronic kidney disease (CKD) is highly prevalent in the general population, little research has been conducted on CKD management in ambulatory care. Objective was to assess management and quality of care by evaluating CKD coding in ambulatory care, patient diagnosis awareness, frequency of monitoring and whether appropriate patients are referred to nephrology.
Methods: Clinical data from the population-based cohort Study of Health in Pomerania (SHIP-START) were matched with claims data of the Association of Statutory Health Insurance Physicians. Quality of care was evaluated according international and German recommendations.
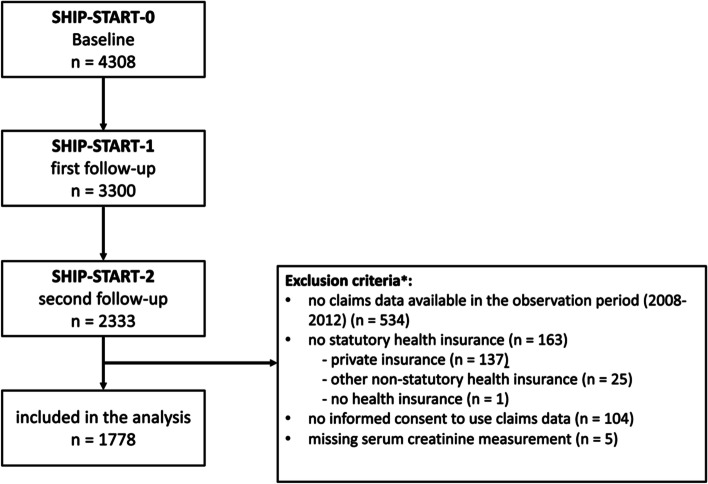
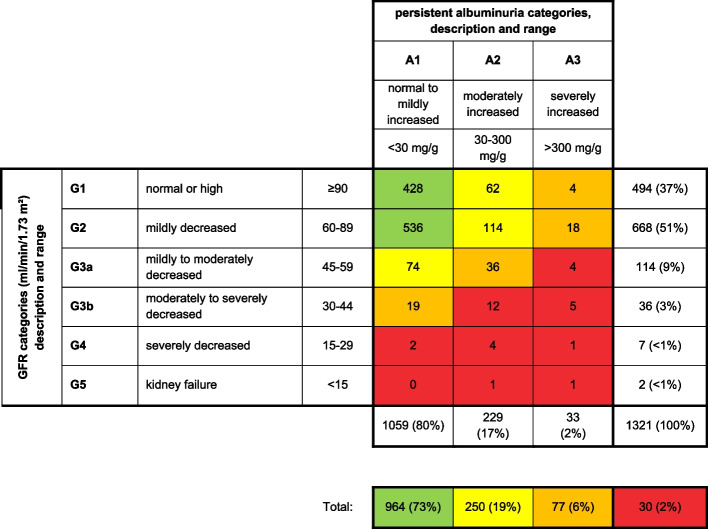
Results: Data from 1778 participants (56% female, mean age 59 years) were analysed. 10% had eGFR < 60 ml/min/1.73m2 (mean age 74 years), 15% had albuminuria. 21% had CKD as defined by KDIGO. 20% of these were coded and 7% self-reported having CKD. Coding increased with GFR stage (G3a 20%, G3b 61%, G4 75%, G5 100%). Serum creatinine and urinary dip stick testing were billed in the majority of all participants regardless of renal function. Testing frequency partially surpassed recommendations. Nephrology consultation was billed in few cases with stage G3b-G4.
Conclusion: CKD coding increased with stage and was performed reliably in stages ≥ G4, while CKD awareness was low. Adherence to monitoring and referral criteria varied, depending on the applicability of monitoring criteria. For assessing quality of care, consent on monitoring, patient education, referral criteria and coordination of care needs to be established, accounting for patient related factors, including age and comorbidity.
Trial registration: This study was prospectively registered as DRKS00009812 in the German Clinical Trials Register (DRKS).
Keywords: Ambulatory care; Chronic kidney disease; Management; Nephrology; Primary care.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
The authors declare that they have no competing interests.
The results presented in this paper have not been published previously in whole or part, except in abstract format.
Figures
Similar articles
-
Health-Related Quality of Life according to Renal Function: Results from a Nationwide Health Interview and Examination Survey.Kidney Blood Press Res. 2022;47(1):13-22. doi: 10.1159/000518668. Epub 2021 Nov 22. Kidney Blood Press Res. 2022. PMID: 34818245 Free PMC article.
-
Prevalence and risk factors for chronic kidney disease in primary health care in the southern region of New Zealand.Nephrology (Carlton). 2019 Mar;24(3):308-315. doi: 10.1111/nep.13395. Nephrology (Carlton). 2019. PMID: 29717528
-
Evaluating the feasibility of the KDIGO CKD referral recommendations.BMC Nephrol. 2017 Jul 7;18(1):223. doi: 10.1186/s12882-017-0646-y. BMC Nephrol. 2017. PMID: 28687072 Free PMC article.
-
Canadian Society of Nephrology commentary on the KDIGO clinical practice guideline for CKD evaluation and management.Am J Kidney Dis. 2015 Feb;65(2):177-205. doi: 10.1053/j.ajkd.2014.10.013. Epub 2014 Nov 4. Am J Kidney Dis. 2015. PMID: 25511161 Review.
-
Diagnosis and management of non-dialysis chronic kidney disease in ambulatory care: a systematic review of clinical practice guidelines.BMC Nephrol. 2018 Oct 11;19(1):258. doi: 10.1186/s12882-018-1048-5. BMC Nephrol. 2018. PMID: 30305035 Free PMC article.
Cited by
-
Obstacles and Opportunities for Albuminuria Testing On the Basis of the Perspective of Primary Care: A Qualitative Study.Clin J Am Soc Nephrol. 2025 Mar 1;20(3):367-376. doi: 10.2215/CJN.0000000620. Epub 2024 Nov 21. Clin J Am Soc Nephrol. 2025. PMID: 39601684
-
General practitioners' assessment and management of chronic kidney disease in older patients- a mixed methods study.BMC Prim Care. 2024 Aug 20;25(1):312. doi: 10.1186/s12875-024-02559-2. BMC Prim Care. 2024. PMID: 39164642 Free PMC article.
-
A retrospective multi-site examination of chronic kidney disease using longitudinal laboratory results and metadata to identify clinical and financial risk.BMC Nephrol. 2024 Dec 6;25(1):447. doi: 10.1186/s12882-024-03869-4. BMC Nephrol. 2024. PMID: 39639199 Free PMC article.
-
General practitioners' representation of early-stage CKD is a barrier to adequate management and patient empowerment: a phenomenological study.J Nephrol. 2024 Mar;37(2):379-390. doi: 10.1007/s40620-023-01838-y. Epub 2024 Jan 16. J Nephrol. 2024. PMID: 38227278
-
Diagnostic Validity of Chronic Kidney Disease in Health Claims Data Over Time: Results from a Cohort of Community-Dwelling Older Adults in Germany.Clin Epidemiol. 2024 Feb 22;16:143-154. doi: 10.2147/CLEP.S438096. eCollection 2024. Clin Epidemiol. 2024. PMID: 38410416 Free PMC article.
References
-
- KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. 2013a;3:1. Available from: https://kdigo.org/wp-content/uploads/2017/02/KDIGO_2012_CKD_GL.pdf. - PubMed
-
- Gergei I, Klotsche J, Woitas RP, Pieper L, Wittchen H-U, Krämer BK, et al. Chronic kidney disease in primary care in Germany. J Public Health. 2017;25:223–230. doi: 10.1007/s10389-016-0773-0. - DOI
-
- Gemeinsame Berichterstattung des Bundes: [Initiation of kidney replacement therapy with haemodialysis, peritoneal dialysis or combined treatment in patients on kidney dialysis.] 2016. Gesundheitsberichterstattung des Bundes, www.gbe-bund.de. Last accessed July 20 2022.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
