

The optimal neoadjuvant chemotherapy regimen for locally advanced gastric and gastroesophageal junction adenocarcinoma: a systematic review and Bayesian network meta-analysis
- PMID: 36352476
- PMCID: PMC9648003
- DOI: 10.1186/s40001-022-00878-7
The optimal neoadjuvant chemotherapy regimen for locally advanced gastric and gastroesophageal junction adenocarcinoma: a systematic review and Bayesian network meta-analysis
Abstract
Background: Neoadjuvant chemotherapy (NAC) for locally advanced gastric and gastroesophageal junction adenocarcinoma (LAGC) has been recommended in several guidelines. However, there is no global consensus about the optimum of NAC regimens. We aimed to determine the optimal NAC regimen for LAGC.
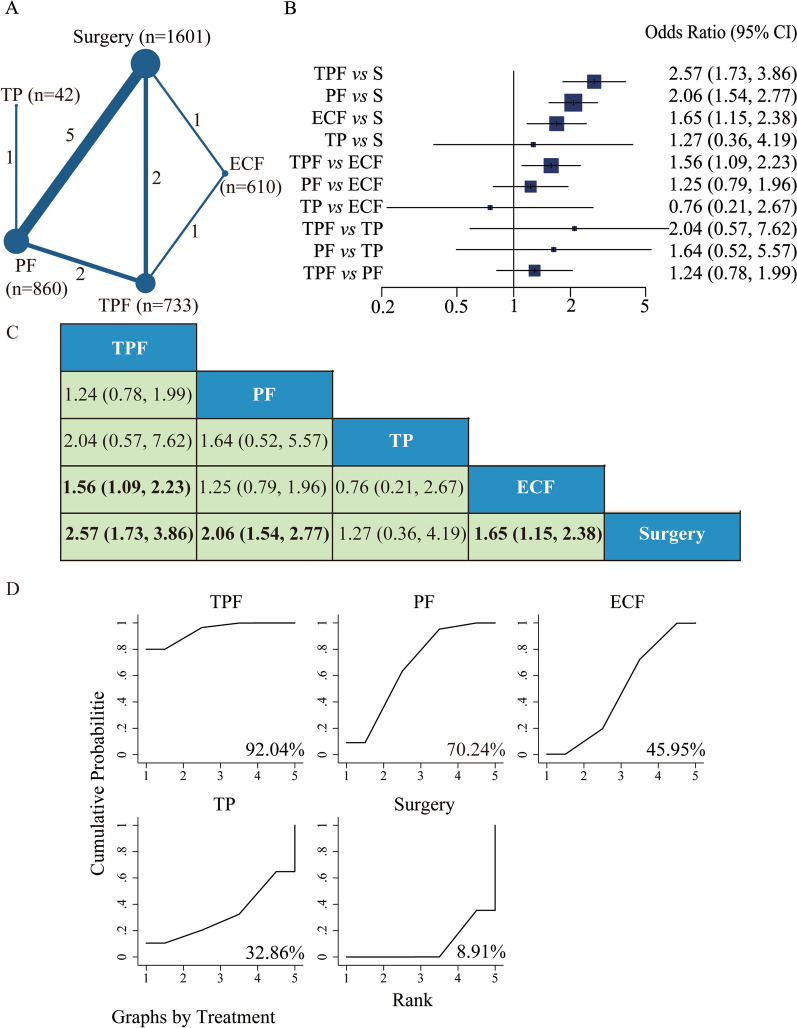
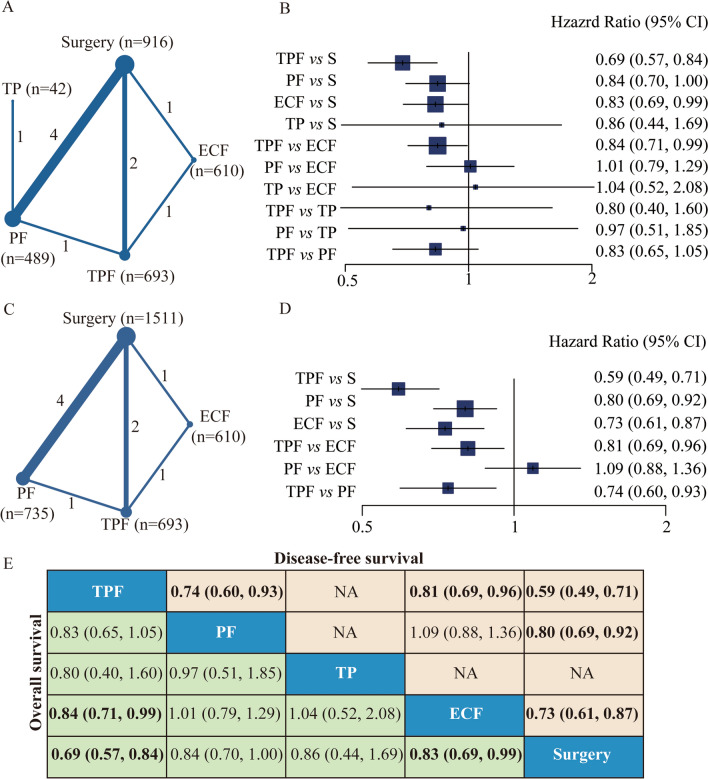
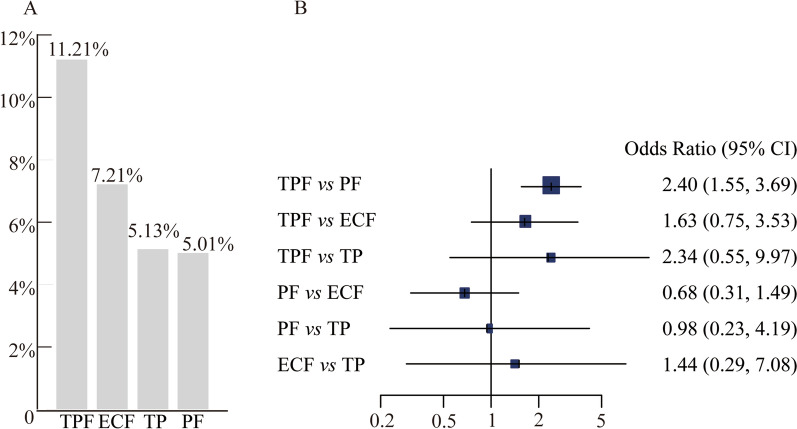
Methods: A systematic review and Bayesian network meta-analysis was performed. The literature search was conducted from inception to June 2022. The odds ratio (OR) value and 95% confidence interval (95% CI) were used for assessment of R0 resection rate and pathological complete response rate (pCR) as primary outcomes. The hazard ratio (HR) value and 95% CI were interpreted for the assessment of overall survival (OS) and disease-free survival (DFS) as second outcomes. The risk ratio (RR) value and 95% CI were used for safety assessment.
Results: Twelve randomized controlled trials were identified with 3846 eligible participants. The network plots for R0 resectability, OS, and DFS constituted closed loops. The regimens of TPF (taxane and platinum plus fluoropyrimidine), ECF (epirubicin and cisplatin plus fluorouracil), and PF (platinum plus fluoropyrimidine) showed a meaningful improvement of R0 resectability, as well as OS and/or DFS, compared with surgery (including surgery-alone and surgery plus postoperative adjuvant chemotherapy). Importantly, among these regimens, TPF regimen showed significant superiority in R0 resection rate (versus ECF regimen), OS (versus ECF regimen), DFS (versus PF and ECF regimens), and pCR (versus PF regimen).
Conclusions: The taxane-based triplet regimen of TPF is likely the optimal neoadjuvant chemotherapy regimen for LAGC patients.
Keywords: Bayesian network meta-analysis; Gastric cancer; Gastroesophageal junction cancer; Neoadjuvant chemotherapy; Systematic review.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Arnold M, Morgan E, Bardot A, Rutherford MJ, Ferlay J, Little A, et al. International variation in oesophageal and gastric cancer survival 2012–2014: differences by histological subtype and stage at diagnosis (an ICBP SURVMARK-2 population-based study) Gut. 2022 doi: 10.1136/gutjnl-2021-325266. - DOI - PubMed
-
- Fujimoto S, Akao T, Itol B, Koshizuka I, Koyano K. A study of survival in patients with stomach cancer treated by a combination of preoperative intra-arterial infusion therapy and surgery. Cancer. 1976;37:1648–1653. - PubMed
-
- Cunningham D, Allum WH, Stenning SP, Thompson JN, Van de Velde CJ, Nicolson M, et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N Eng J Med. 2006;355(1):11–20. - PubMed
-
- NCCN Clinical Practice Guidelines in Oncology. 2007 Gastric Cancer. V.1(10).
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
