

Proposed strategies to overcome venous occlusion in the implantation of a cardiac implantable electronic device: A case report and literature review
- PMID: 36352849
- PMCID: PMC9637934
- DOI: 10.3389/fcvm.2022.1005596
Proposed strategies to overcome venous occlusion in the implantation of a cardiac implantable electronic device: A case report and literature review
Abstract
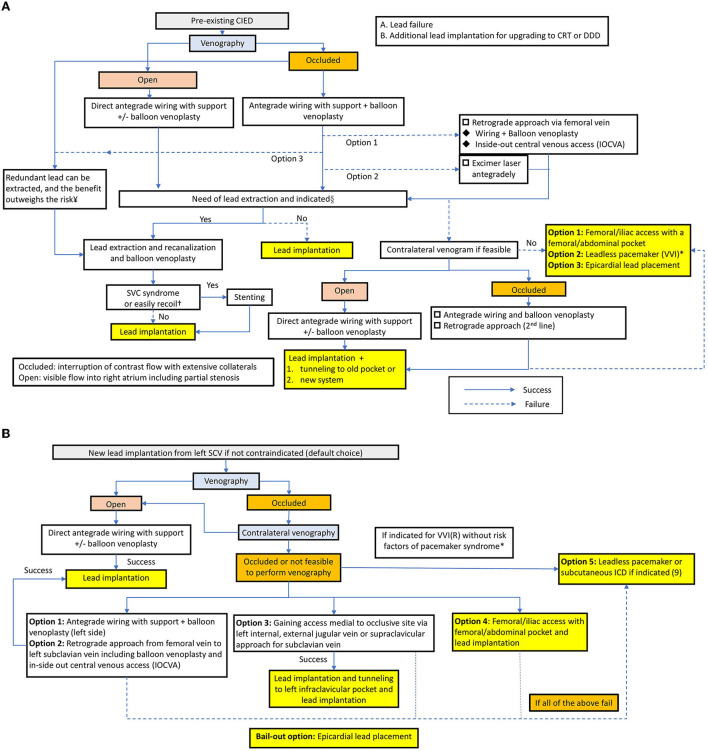
This case report describes a successful balloon venoplasty to overcome a total occlusion from the brachiocephalic vein to the superior vena cava in a patient undergoing cardiac resynchronization therapy. It is crucial for implanting physicians to be familiar with strategies to overcome venous occlusion in lead implantation, especially balloon venoplasty, which is an effective and safe approach.
Keywords: balloon venoplasty; cardiac implantable electronic device; cardiac synchronization therapy; pacemaker; venous occlusion.
Copyright © 2022 Li, Lee and Chen.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures


References
Publication types
LinkOut - more resources
Full Text Sources