

Lip pleomorphic adenomas: case series and literature review
- PMID: 36353586
- PMCID: PMC9638788
- DOI: 10.21037/gs-22-308
Lip pleomorphic adenomas: case series and literature review
Abstract
Background: Pleomorphic adenoma (PA) is the most frequent benign salivary gland tumor, but a lip PA is rare. Although this tumor may be definitively diagnosed by imaging or a tissue biopsy if it is reasonably large, PAs on the lip are relatively small, and they present findings that are similar to those of other lip lesions, which can make a preoperative diagnosis difficult.
Methods: We analyzed all PAs in the oral region and lesions on the lips treated in our department over the past 20 years, and we discuss them together with the relevant literature.
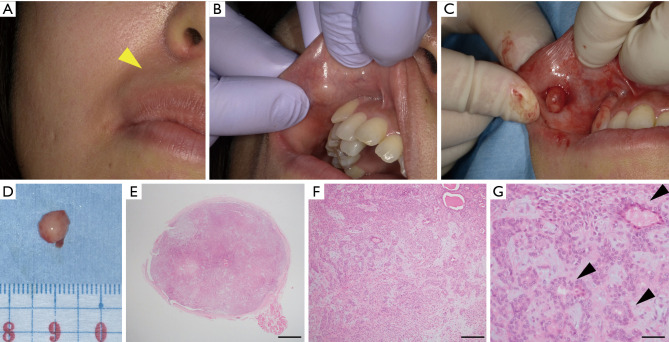
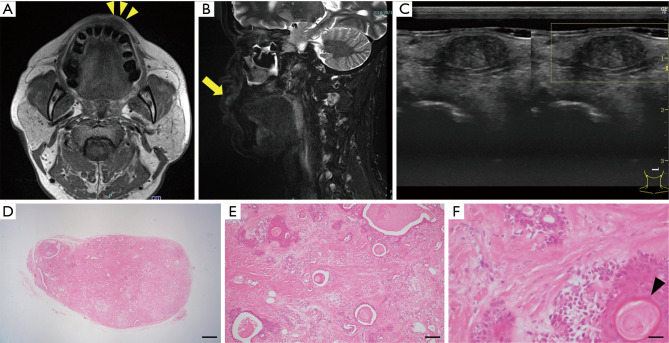
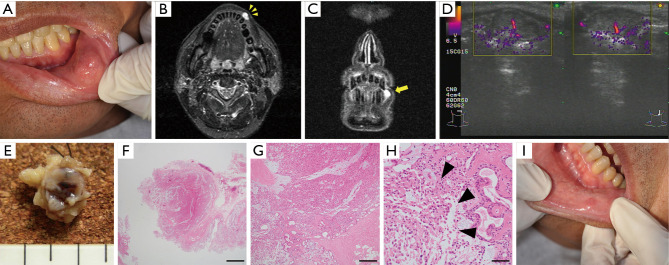
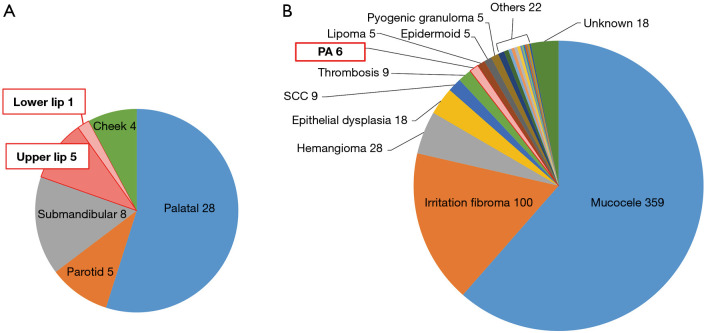
Results: We found that 11.8% (n=6) of the PAs occurred on a lip (upper lip: 9.8%, lower lip: 2.0%), and ~1% of all mass lesions of the lips were PAs. The average size of the lip PAs was 1.5±0.7 cm (range, 0.7-2.2 cm). For preoperative diagnostic assistance, ultrasonography (US) (n=4), magnetic resonance (MR) (n=3), or no imaging (n=2) was used. An excisional biopsy was performed in all cases, and to date, no recurrence or malignant transformation has been observed.
Conclusions: Lip PA is relatively rare. Because almost all of these lesions are small, a preoperative diagnosis is more difficult compared to palatal lesions. This tumor is also prone to long-term neglect and has the potential for recurrence and malignant transformation. It is thus necessary to perform an excision that includes the capsule and surrounding tissues, and careful postoperative follow-up should be continued.
Keywords: Pleomorphic adenoma (PA); case series; lower lip; minor salivary gland tumor; upper lip.
2022 Gland Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://gs.amegroups.com/article/view/10.21037/gs-22-308/coif). The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Pleomorphic adenoma (mixed tumor) of the upper lip: A case report.World J Clin Cases. 2024 Jun 16;12(17):3138-3143. doi: 10.12998/wjcc.v12.i17.3138. World J Clin Cases. 2024. PMID: 38898865 Free PMC article.
-
Pleomorphic adenoma of the lip: a case report and literature review.J Surg Case Rep. 2025 May 15;2025(5):rjaf311. doi: 10.1093/jscr/rjaf311. eCollection 2025 May. J Surg Case Rep. 2025. PMID: 40376544 Free PMC article.
-
Pleomorphic Adenoma of the Upper Lip: A Case Report.Saudi J Med Med Sci. 2018 Jan-Apr;6(1):32-35. doi: 10.4103/sjmms.sjmms_109_16. Epub 2017 Dec 14. Saudi J Med Med Sci. 2018. PMID: 30787814 Free PMC article.
-
Comprehensive characterization of pleomorphic adenoma at intraoral unusual sites.Oral Surg Oral Med Oral Pathol Oral Radiol. 2022 Jan;133(1):21-27. doi: 10.1016/j.oooo.2021.05.006. Epub 2021 May 24. Oral Surg Oral Med Oral Pathol Oral Radiol. 2022. PMID: 34511341 Review.
-
Aspiration cytology of pleomorphic adenoma with squamous metaplasia: A case series and literature review illustrating diagnostic challenges.Diagn Cytopathol. 2022 Feb;50(2):64-74. doi: 10.1002/dc.24915. Epub 2021 Dec 20. Diagn Cytopathol. 2022. PMID: 34927804 Review.
Cited by
-
An unusual exophytic pleomorphic adenoma on the upper lip skin without mucosa involvement: a case report.Arch Craniofac Surg. 2024 Aug;25(4):201-204. doi: 10.7181/acfs.2023.00626. Epub 2024 Jul 18. Arch Craniofac Surg. 2024. PMID: 39020470 Free PMC article.
-
Pleomorphic adenoma (mixed tumor) of the upper lip: A case report.World J Clin Cases. 2024 Jun 16;12(17):3138-3143. doi: 10.12998/wjcc.v12.i17.3138. World J Clin Cases. 2024. PMID: 38898865 Free PMC article.
-
Pleomorphic adenoma of the lip: a case report and literature review.J Surg Case Rep. 2025 May 15;2025(5):rjaf311. doi: 10.1093/jscr/rjaf311. eCollection 2025 May. J Surg Case Rep. 2025. PMID: 40376544 Free PMC article.
References
-
- Neville B. Oral and maxillofacial pathology. 3rd edition. Saunders, 2003:477-80,93-95.
LinkOut - more resources
Full Text Sources
Miscellaneous