

Accuracy of a Three-Dimensional (3D)-Printed Patient-Specific (PS) Femoral Osteotomy Guide: A Computed Tomography (CT) Study
- PMID: 36354578
- PMCID: PMC9687720
- DOI: 10.3390/bioengineering9110667
Accuracy of a Three-Dimensional (3D)-Printed Patient-Specific (PS) Femoral Osteotomy Guide: A Computed Tomography (CT) Study
Abstract
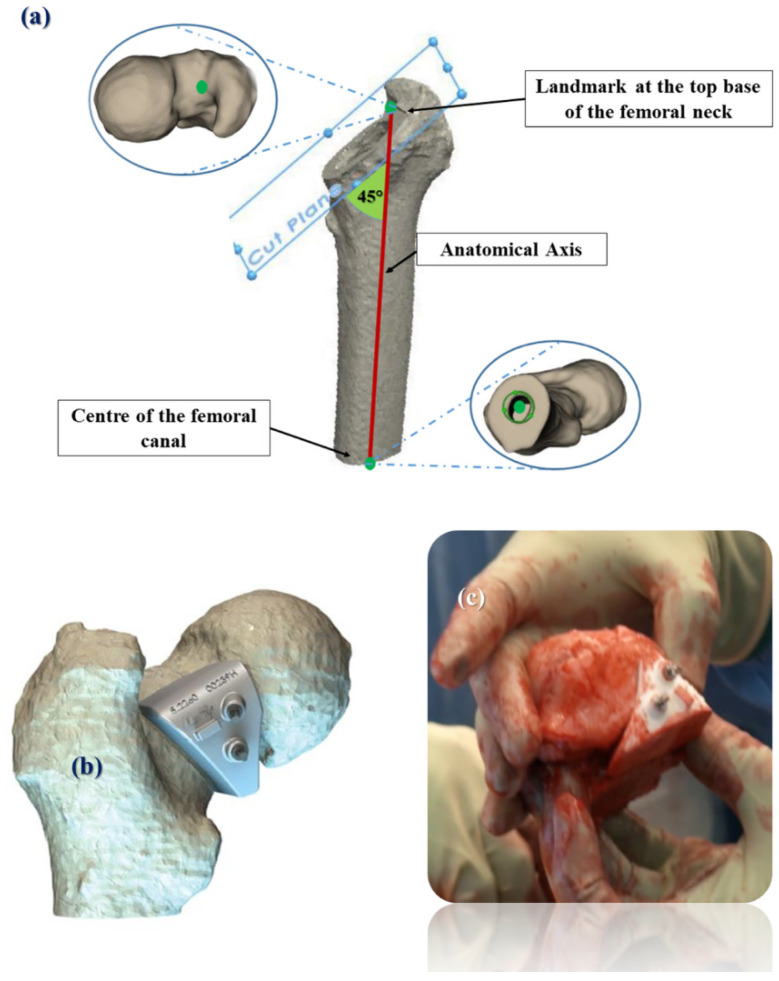
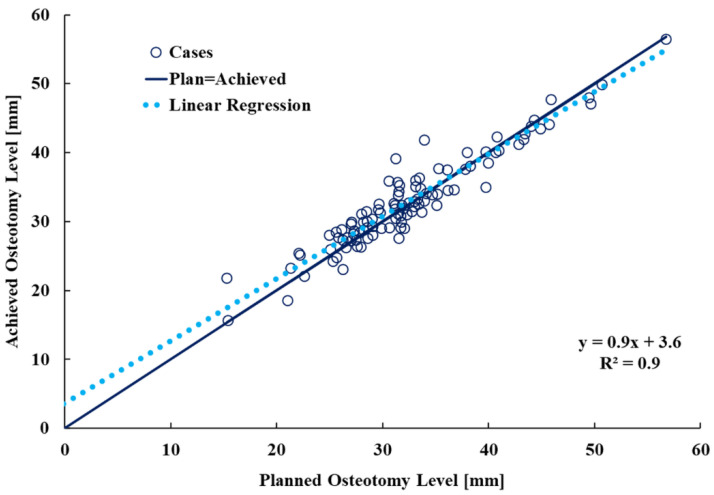
Femoral neck osteotomy creates a critical anatomical landmark for surgeons performing primary Total Hip Arthroplasty (THA); it affects the final height and position of the femoral component. Patient Specific Instrumentation (PSI) has been developed to guide the osteotomy. We aimed to assess the accuracy of a patient-specific (PS) femoral osteotomy guide in primary THA using three-dimensional (3D) computed tomography (CT) analysis. We included pre- and post-operative CT data of 103 THAs. All patients underwent 3D planning to define the optimal femoral neck osteotomy level. Our primary objective was to quantify the discrepancy between the achieved and planned osteotomy level; our secondary objective was to evaluate the clinical outcome. The median (Interquartile Range—IQR) discrepancy between the achieved and planned osteotomy level was 0.3 mm (−1 mm to 2 mm). We found a strong positive correlation between the planned and achieved osteotomy level (R2 = 0.9, p < 0.001). A satisfactory clinical outcome was recorded. Our findings suggest that surgeons can use 3D-printed PS guides to achieve a femoral neck osteotomy with a high level of accuracy to the plan.
Keywords: 3D-printed patient-specific guides; femoral neck osteotomy; total hip arthroplasty.
Conflict of interest statement
One author declares institutional funding not directly related to this work. The other authors declare no conflict of interest relevant to this work.
Figures






References
LinkOut - more resources
Full Text Sources
