

Cranial Radiation Therapy as Salvage in the Treatment of Relapsed Primary CNS Lymphoma
- PMID: 36354704
- PMCID: PMC9689217
- DOI: 10.3390/curroncol29110644
Cranial Radiation Therapy as Salvage in the Treatment of Relapsed Primary CNS Lymphoma
Abstract
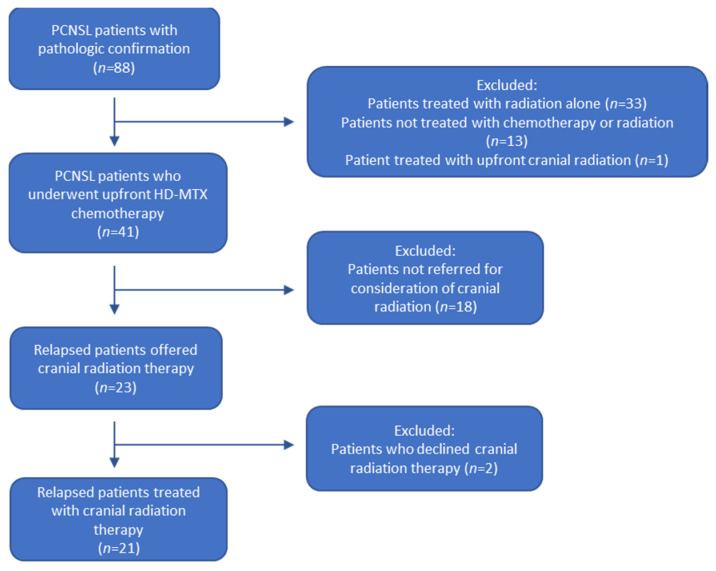
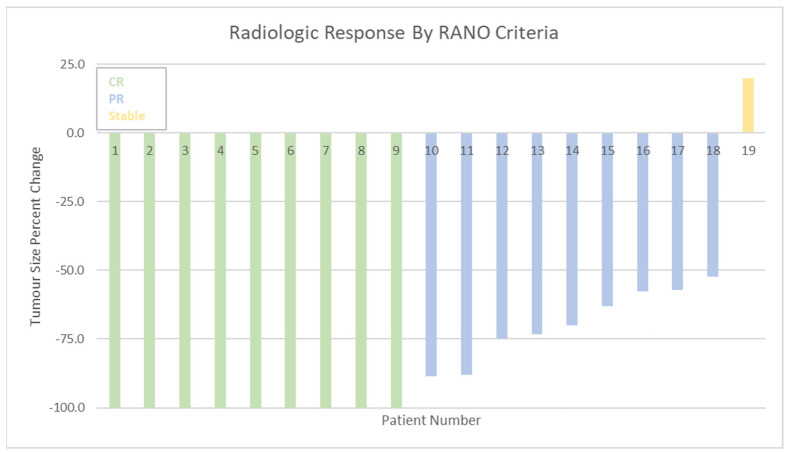
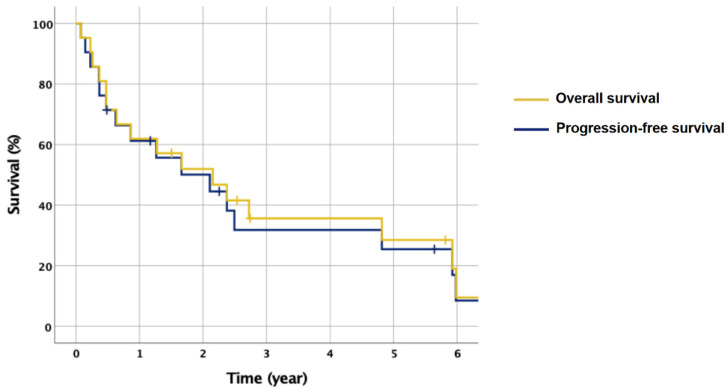
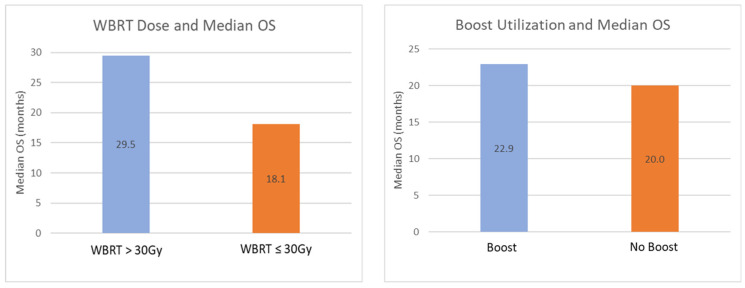
Primary central nervous system lymphoma (PCNSL) is a rare malignancy. Standard of care is upfront high-dose methotrexate (HD-MTX) chemotherapy, while cranial radiation is more commonly used in the salvage setting. In this retrospective study, we aimed to investigate the safety and efficacy of salvage cranial radiation in PCNSL. PCNSL patients who received upfront HD-MTX chemotherapy and salvage cranial radiation after treatment failure between 1995 and 2018 were selected. Radiological response to cranial radiation was assessed as per Response Assessment in Neuro-Oncology Criteria. Twenty one patients were selected (median age 59.9 years), with median follow-up of 19.9 months. Fourteen patients (66.7%) received a boost to the gross tumour volume (GTV). Four patients (19.0%) sustained grade ≥2 treatment-related neurotoxicity post-completion of cranial radiation. Of the 19 patients who had requisite MRI with gadolinium imaging available for Response Assessment in Neuro-Oncology (RANO) criteria assessment, 47.4% achieved complete response, 47.4% achieved partial response, and 5.3% of patients exhibited stable disease. Higher dose to the whole brain (>30 Gy) was associated with higher rate of complete response (63.6%) than lower dose (≤30 Gy, 37.5%), while boost dose to the gross disease was also associated with higher rate of complete response (61.5%) compared with no boost dose (33.3%). Median overall survival was 20.0 months. PCNSL patients who relapsed following upfront chemotherapy showed a high rate of response to salvage cranial radiation, especially in those receiving greater than 30 Gy to the whole brain and boost to gross disease.
Keywords: cranial radiation therapy; primary CNS lymphoma; salvage radiation therapy; whole brain radiation therapy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Nelson D.F., Martz K.L., Bonner H., Nelson J.S., Newall J., Kerman H.D., Thomson J.W., Murray K.J. Non-Hodgkin’s lymphoma of the brain: Can high dose, large volume radiation therapy improve survival? Report on a prospective trial by the Radiation Therapy Oncology Group (RTOG): RTOG 8315. Int. J. Radiat. Oncol. Biol. Phys. 1992;23:9–17. doi: 10.1016/0360-3016(92)90538-S. - DOI - PubMed
-
- Ferreri A.J., Reni M., Dell’Oro S., Ciceri F., Bernardi M., Camba L., Ponzoni M., Terreni M.R., Tomirotti M., Spina M., et al. Combined treatment with high-dose methotrexate, vincristine and procarbazine, without intrathecal chemotherapy, followed by consolidation radiotherapy for primary central nervous system lymphoma in immunocompetent patients. Oncology. 2001;60:134–140. doi: 10.1159/000055310. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
