

Vaccine-hesitant individuals accumulate additional COVID-19 risk due to divergent perception and behaviors related to SARS-CoV-2 testing: a population-based, cross-sectional study
- PMID: 36355269
- PMCID: PMC9647754
- DOI: 10.1007/s15010-022-01947-z
Vaccine-hesitant individuals accumulate additional COVID-19 risk due to divergent perception and behaviors related to SARS-CoV-2 testing: a population-based, cross-sectional study
Abstract
Purpose: To investigate the perception of SARS-CoV-2 detection methods, information sources, and opinions on appropriate behavior after receiving negative or positive test results.
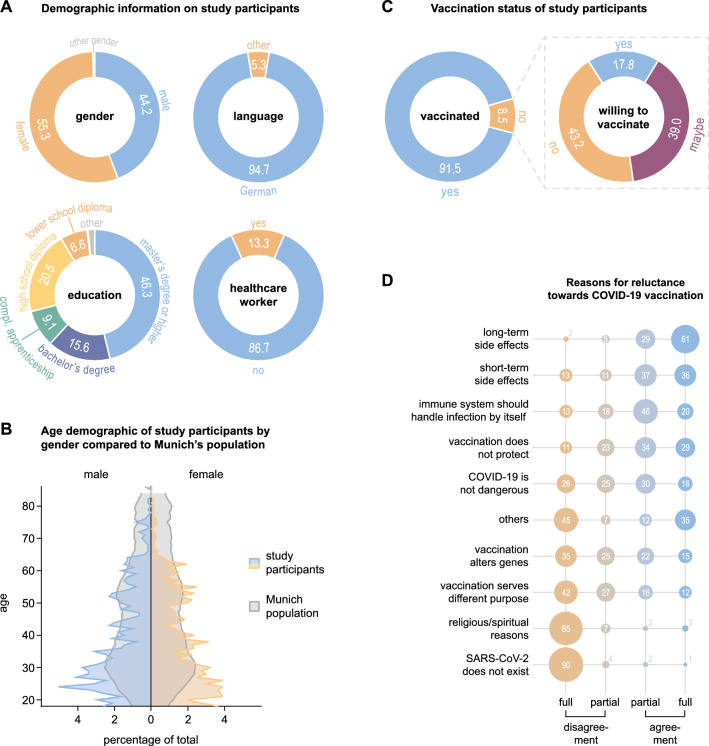
Methods: In a questionnaire-based, cross-sectional study conducted between September 1 and November 17, 2021, epidemiological, behavioral, and COVID-19-related data were acquired from the public in Munich, Germany.
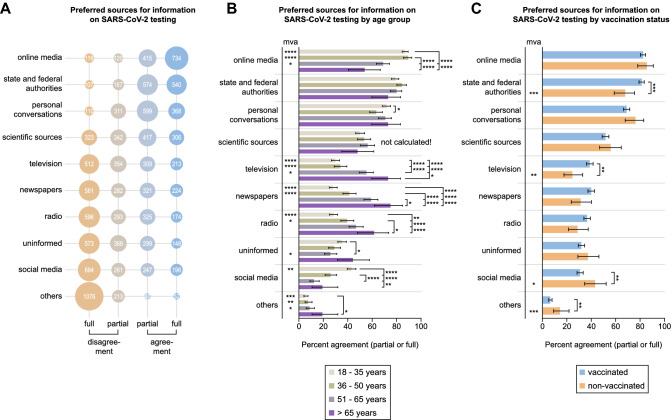
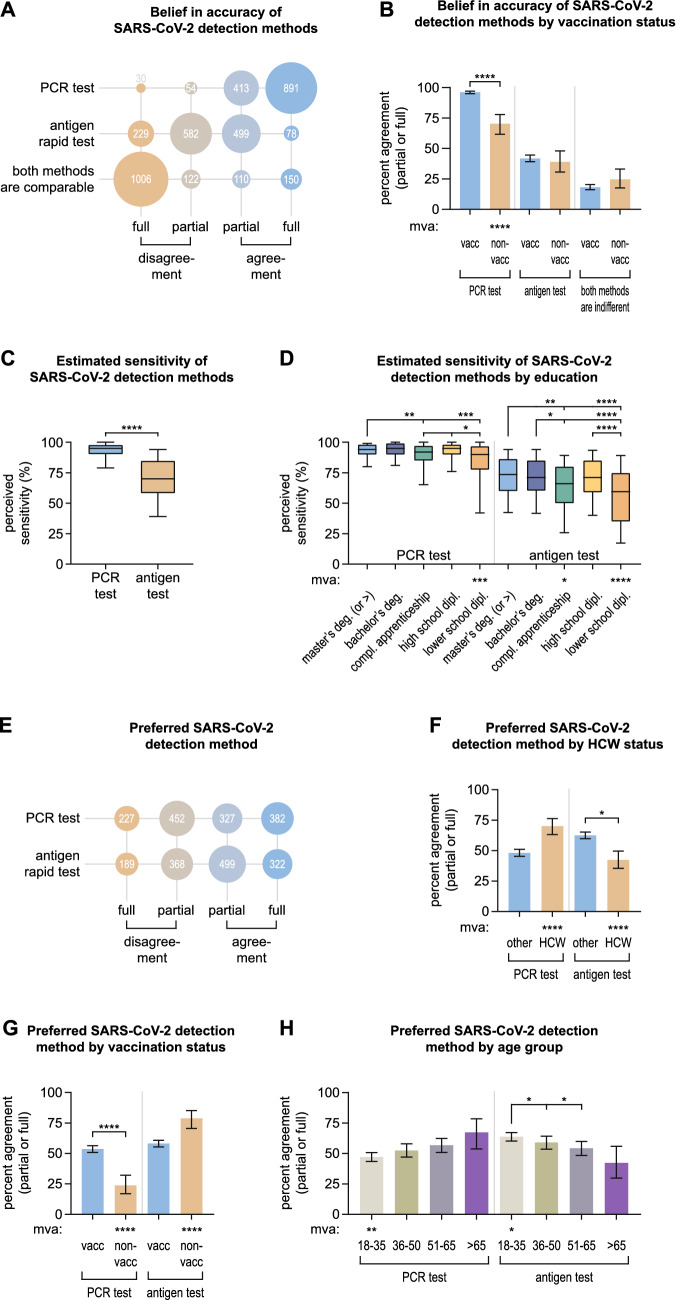
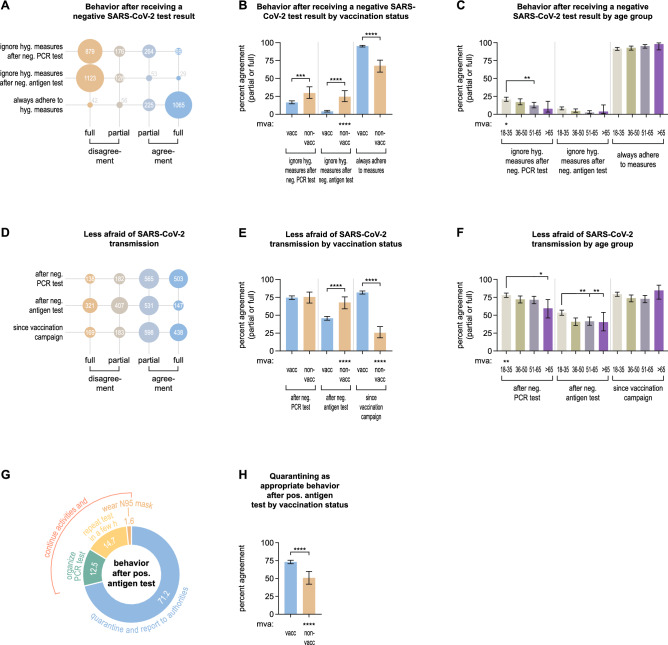
Results: Most of the 1388 participants obtained information from online media (82.8%) as well as state and federal authorities (80.3%). 93.4% believed in the accuracy of SARS-CoV-2 PCR testing and 41.2% in the accuracy of rapid antigen tests (RATs). However, RATs were preferred for testing (59.1%) over PCR (51.1%). 24.0% of all individuals were willing to ignore hygiene measures and 76.9% were less afraid of SARS-CoV-2 transmission after receiving a negative PCR test (5.9% and 48.8% in case of a negative RAT). 28.8% reported not to self-isolate after receiving a positive RAT. Multivariate analyses revealed that non-vaccinated individuals relied less on information from governmental authorities (p = 0.0004) and more on social media (p = 0.0216), disbelieved in the accuracy of the PCR test (p ≤ 0.0001) while displaying strong preference towards using RATs (p ≤ 0.0001), were more willing to abandon pandemic-related hygiene measures (p ≤ 0.0001), less afraid of transmitting SARS-CoV-2 after a negative RAT (p ≤ 0.0001), and less likely to isolate after a positive RAT (p ≤ 0.0001).
Conclusion: Insights into preferred information sources as well as perception, preferences, and behavior related to SARS-CoV-2 testing and hygiene measures are key to refining public health information and surveillance campaigns. Non-vaccinated individuals' divergent believes and behaviors possibly increase their COVID-19 risk.
Keywords: COVID-19; PCR test; Rapid antigen test; SARS-CoV-2; Surveillance; Vaccination.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Effectiveness and cost-effectiveness of four different strategies for SARS-CoV-2 surveillance in the general population (CoV-Surv Study): a structured summary of a study protocol for a cluster-randomised, two-factorial controlled trial.Trials. 2021 Jan 8;22(1):39. doi: 10.1186/s13063-020-04982-z. Trials. 2021. PMID: 33419461 Free PMC article.
-
Mass Screening of SARS-CoV-2 With Rapid Antigen Tests in a Receding Omicron Wave: Population-Based Survey for Epidemiologic Evaluation.JMIR Public Health Surveill. 2022 Nov 9;8(11):e40175. doi: 10.2196/40175. JMIR Public Health Surveill. 2022. PMID: 36240027 Free PMC article.
-
Values and preferences of the general population in Indonesia in relation to rapid COVID-19 antigen self-tests: A cross-sectional survey.Trop Med Int Health. 2022 May;27(5):522-536. doi: 10.1111/tmi.13748. Epub 2022 Apr 5. Trop Med Int Health. 2022. PMID: 35332616 Free PMC article.
-
SARS-CoV-2 self-testing in Peru: a cross-sectional survey of values and attitudes of the general population.BMJ Open. 2023 Jul 5;13(7):e068980. doi: 10.1136/bmjopen-2022-068980. BMJ Open. 2023. PMID: 37407037 Free PMC article.
-
Who is hesitant about Covid-19 vaccines? The profiling of participants in a French online cohort.Rev Epidemiol Sante Publique. 2022 Jun;70(3):123-131. doi: 10.1016/j.respe.2022.02.004. Epub 2022 Mar 28. Rev Epidemiol Sante Publique. 2022. PMID: 35428543 Free PMC article.
Cited by
-
A network-based model to assess vaccination strategies for the COVID-19 pandemic by using Bayesian optimization.Chaos Solitons Fractals. 2024 Apr;181:114695. doi: 10.1016/j.chaos.2024.114695. Epub 2024 Mar 14. Chaos Solitons Fractals. 2024. PMID: 40822278 Free PMC article.
-
Ten rapid antigen tests for SARS-CoV-2 widely differ in their ability to detect Omicron-BA.4 and -BA.5.Med Microbiol Immunol. 2023 Oct;212(5):323-337. doi: 10.1007/s00430-023-00775-8. Epub 2023 Aug 10. Med Microbiol Immunol. 2023. PMID: 37561225 Free PMC article.
-
Impact of unequal testing on vaccine effectiveness estimates across two study designs: a simulation study.Nat Commun. 2025 May 24;16(1):4849. doi: 10.1038/s41467-025-59768-1. Nat Commun. 2025. PMID: 40413178 Free PMC article.
-
Dietary habits, traveling and the living situation potentially influence the susceptibility to SARS-CoV-2 infection: results from healthcare workers participating in the RisCoin Study.Infection. 2024 Aug;52(4):1425-1437. doi: 10.1007/s15010-024-02201-4. Epub 2024 Mar 4. Infection. 2024. PMID: 38436913 Free PMC article.
-
Effective surveillance of acute COVID-19 using a cost- and labor-efficient approach: a paradigm for the longitudinal monitoring of respiratory infections in larger cohorts.Infection. 2025 May 12. doi: 10.1007/s15010-025-02526-8. Online ahead of print. Infection. 2025. PMID: 40354031
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
