

Formation and Fixation of the Annulus of Zinn and Relation With Extraocular Muscles: A Plastinated Histologic Study and Its Clinical Significance
- PMID: 36355368
- PMCID: PMC9652724
- DOI: 10.1167/iovs.63.12.16
Formation and Fixation of the Annulus of Zinn and Relation With Extraocular Muscles: A Plastinated Histologic Study and Its Clinical Significance
Abstract
Purpose: This study aimed to clarify the formation and fixation of the annulus of Zinn (AZ) and its relationship with the extraocular muscles by using ultrathin plastination and three-dimensional models.
Methods: Eighteen cadaveric heads (36 sides of the orbital apex) were plastinated to coronal (16 sides), sagittal (13 sides), and horizontal (5 sides) ultrathin plastination sections to be investigated at both macroscopic and microscopic levels. One cadaveric head was used for endoscopic dissection to identify anatomic landmarks.
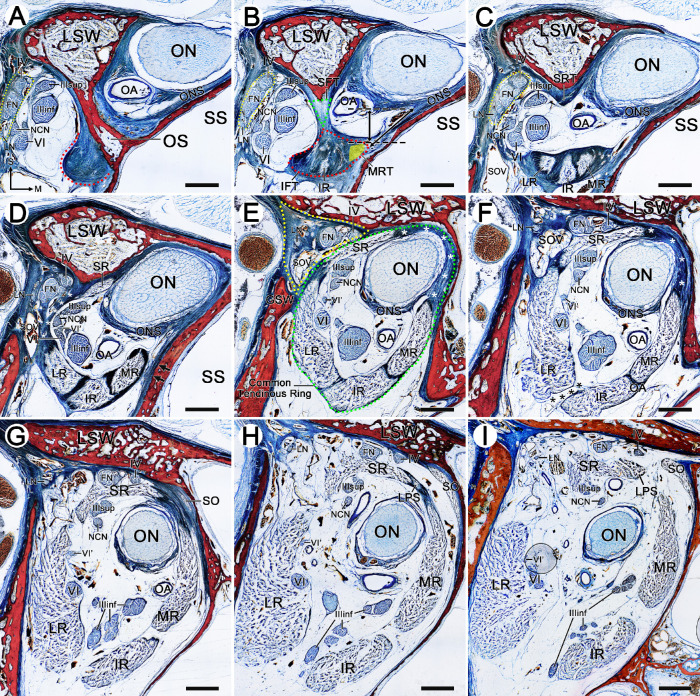
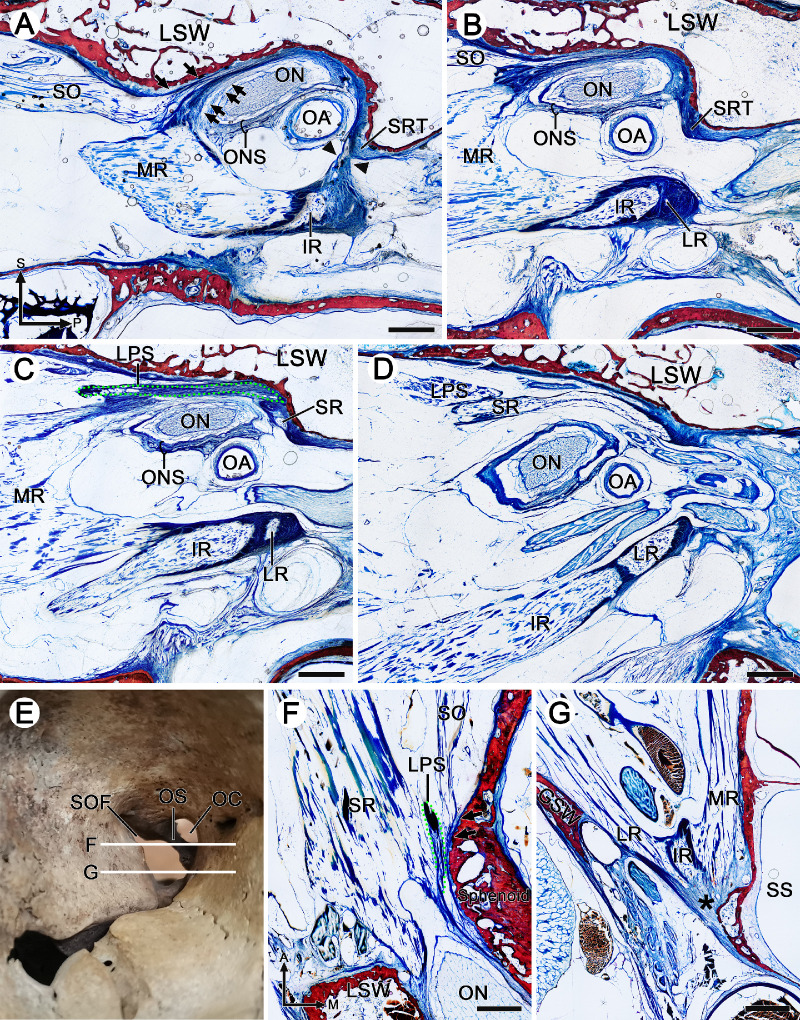
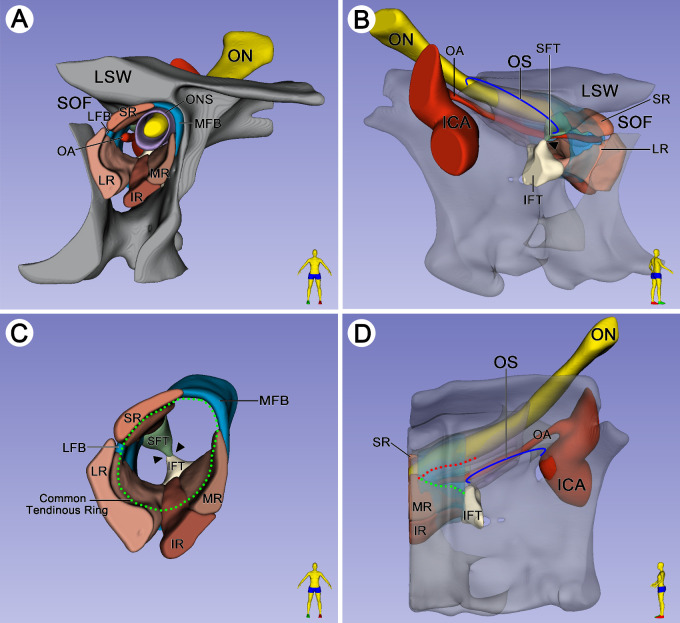
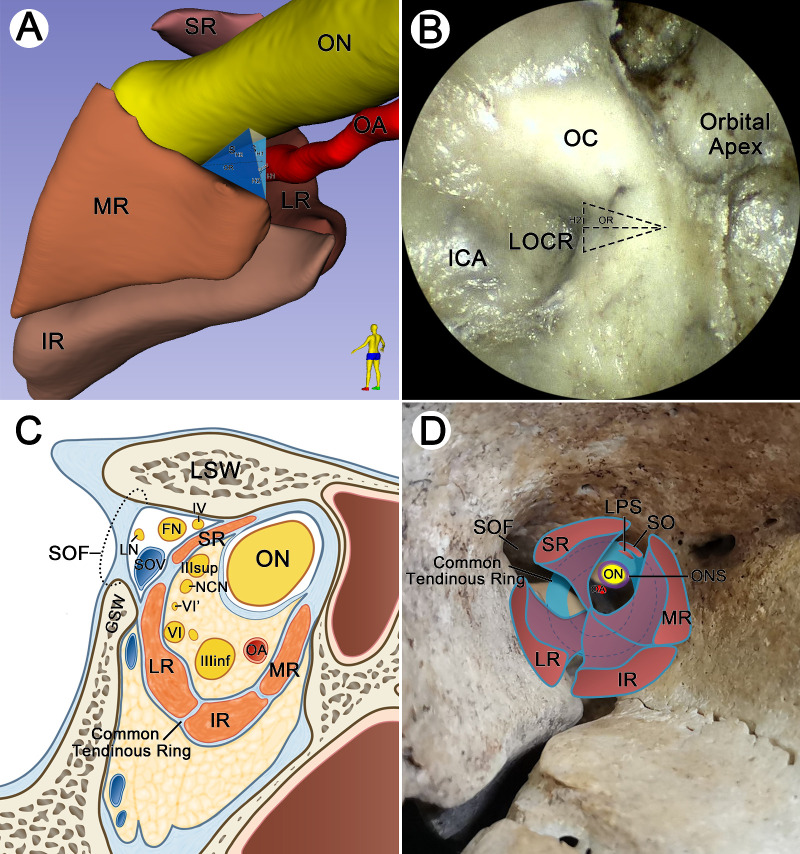
Results: There were two fibrous triangles adhered to both ends of the anterior surface of the optic strut. The superior rectus muscle originated from the superior fibrous triangle, and the lateral, inferior, and medial rectus muscles emerged from the inferior fibrous triangle. It was not until 5.46 ± 0.41 mm anterior to the optic strut that the complete tendinous ring composed of rectus muscles, optic nerve sheath, and periosteum was formed. The superior oblique and levator palpebrae superioris muscles originated from the medial fibrous band of the AZ. At the posterior of the AZ, there was a potential passage between the medial rectus muscle and the optic nerve.
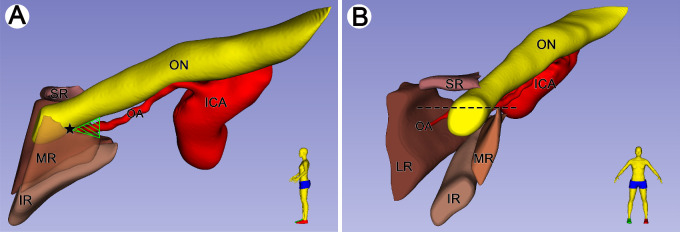
Conclusions: The fixation of the AZ was composed of the connection of the annular tendon to the optic strut posteriorly and the attachment of the complete tendinous ring to the lesser and greater wings of the sphenoid bone anteriorly. The triangular route area between the optic nerve and medial rectus muscle was located on the anterior side of the base of the optic strut.
Conflict of interest statement
Disclosure:
Figures
Similar articles
-
Tendinous annulus of Zinn for a common origin of the extraocular rectus muscles: a histological study of the orbital apex from donated elderly cadavers.Anat Sci Int. 2022 Sep;97(4):369-379. doi: 10.1007/s12565-022-00649-8. Epub 2022 Feb 14. Anat Sci Int. 2022. PMID: 35157253
-
Anatomy, Head and Neck, Orbit Bones.2023 Jul 24. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2023 Jul 24. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30285385 Free Books & Documents.
-
The origins and insertions of the extraocular muscles: development, histologic features, and clinical significance.Trans Am Ophthalmol Soc. 1986;84:488-526. Trans Am Ophthalmol Soc. 1986. PMID: 3590478 Free PMC article.
-
Examination of the Topographical Anatomy and Fetal Development of the Tendinous Annulus of Zinn for a Common Origin of the Extraocular Recti.Invest Ophthalmol Vis Sci. 2019 Nov 1;60(14):4564-4573. doi: 10.1167/iovs.19-28094. Invest Ophthalmol Vis Sci. 2019. PMID: 31675425
-
Double insertions of extraocular rectus muscles in humans and the pulley theory.J Anat. 2005 Mar;206(3):295-306. doi: 10.1111/j.1469-7580.2005.00383.x. J Anat. 2005. PMID: 15733302 Free PMC article. Review.
Cited by
-
Microsurgical Anatomy of the Common Tendinous Ring and Its Surgical Implications.Oper Neurosurg. 2025 Jun 1;28(6):862-871. doi: 10.1227/ons.0000000000001377. Epub 2024 Sep 23. Oper Neurosurg. 2025. PMID: 39311609
-
Unveiling the vulnerability of the human abducens nerve: insights from comparative cranial base anatomy in mammals and primates.Front Neuroanat. 2024 Apr 29;18:1383126. doi: 10.3389/fnana.2024.1383126. eCollection 2024. Front Neuroanat. 2024. PMID: 38741761 Free PMC article.
References
-
- Standring S. Gray's Anatomy: The Anatomical Basis of Clinical Practice. 41st ed. London, UK: Churchill Livingstone; 2015: 668–670.
-
- Lin J, Hu W, Wu Q, Zhang J, Yan W.. An evolving perspective of endoscopic transnasal optic canal decompression for traumatic optic neuropathy in clinic. Neurosurg Rev. 2021; 44(1): 19–27. - PubMed
-
- Chen B, Zhang H, Zhai Q, Li H, Wang C, Wang Y.. Traumatic optic neuropathy: a review of current studies. Neurosurg Rev. 2022; 45(3): 1895–1913. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
