

Variation in aorta attenuation in contrast-enhanced CT and its implications for calcification thresholds
- PMID: 36355794
- PMCID: PMC9648778
- DOI: 10.1371/journal.pone.0277111
Variation in aorta attenuation in contrast-enhanced CT and its implications for calcification thresholds
Abstract
Background: CT contrast media improves vessel visualization but can also confound calcification measurements. We evaluated variance in aorta attenuation from varied contrast-enhancement scans, and quantified expected plaque detection errors when thresholding for calcification.
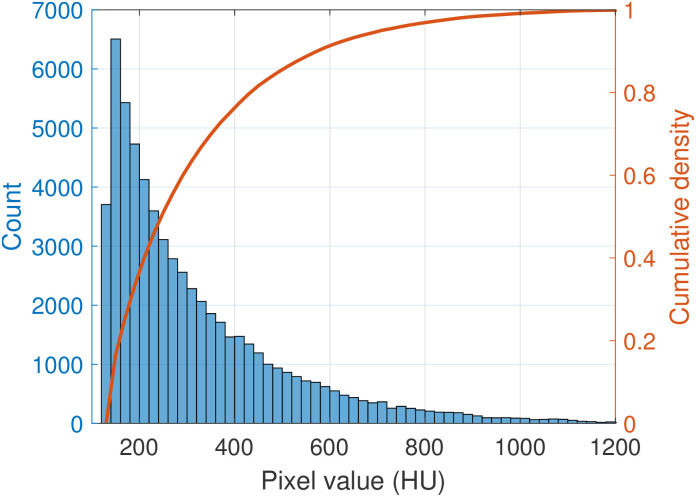
Methods: We measured aorta attenuation (AoHU) in central vessel regions from 10K abdominal CT scans and report AoHU relationships to contrast phase (non-contrast, arterial, venous, delayed), demographic variables (age, sex, weight), body location, and scan slice thickness. We also report expected plaque segmentation false-negative errors (plaque pixels misidentified as non-plaque pixels) and false-positive errors (vessel pixels falsely identified as plaque), comparing a uniform thresholding approach and a dynamic approach based on local mean/SD aorta attenuation.
Results: Females had higher AoHU than males in contrast-enhanced scans by 65/22/20 HU for arterial/venous/delayed phases (p < 0.001) but not in non-contrast scans (p > 0.05). Weight was negatively correlated with AoHU by 2.3HU/10kg but other predictors explained only small portions of intra-cohort variance (R2 < 0.1 in contrast-enhanced scans). Average AoHU differed by contrast phase, but considerable overlap was seen between distributions. Increasing uniform plaque thresholds from 130HU to 200HU/300HU/400HU produces respective false-negative plaque content losses of 35%/60%/75% from all scans with corresponding false-positive errors in arterial-phase scans of 95%/60%/15%. Dynamic segmentation at 3SD above mean AoHU reduces false-positive errors to 0.13% and false-negative errors to 8%, 25%, and 70% in delayed, venous, and arterial scans, respectively.
Conclusion: CT contrast produces heterogeneous aortic enhancements not readily determined by demographic or scan protocol factors. Uniform CT thresholds for calcified plaques incur high rates of pixel classification errors in contrast-enhanced scans which can be minimized using dynamic thresholds based on local aorta attenuation. Care should be taken to address these errors and sex-based biases in baseline attenuation when designing automatic calcification detection algorithms intended for broad use in contrast-enhanced CTs.
Copyright: © 2022 Holcombe et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures






References
-
- Virani Salim S, Alonso Alvaro, Aparicio Hugo J, Benjamin Emelia J, Bittencourt Marcio S, Callaway Clifton W, et al.. Heart Disease and Stroke Statistics—2021 Update. Circulation. 2021;143(8):e254–e743. - PubMed
-
- Greenland P, Alpert JS, Beller GA, Benjamin EJ, Budoff MJ, Fayad ZA, et al.. 2010 ACCF/AHA guideline for assessment of cardiovascular risk in asymptomatic adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Journal of the American College of Cardiology. 2010;56(25):e50–103. doi: 10.1016/j.jacc.2010.09.001 - DOI - PubMed
-
- Ong KL, McClelland RL, Rye KA, Cheung BMY, Post WS, Vaidya D, et al.. The relationship between insulin resistance and vascular calcification in coronary arteries, and the thoracic and abdominal aorta: The Multi-Ethnic Study of Atherosclerosis. Atherosclerosis. 2014;236(2):257–262. doi: 10.1016/j.atherosclerosis.2014.07.015 - DOI - PMC - PubMed
-
- Wilson PWF, O’Donnell CJ. Epidemiology of Chronic Coronary Artery Disease. In: Chronic Coronary Artery Disease: A Companion to Braunwald’s Heart Disease. 1st ed. Elsevier, Inc; 2017. p. 1–15. Available from: https://www.elsevier.com/books/chronic-coronary-artery-disease/de-lemos/....
-
- Pickhardt PJ, Graffy PM, Zea R, Lee SJ, Liu J, Sandfort V, et al.. Automated CT biomarkers for opportunistic prediction of future cardiovascular events and mortality in an asymptomatic screening population: a retrospective cohort study. The Lancet Digital Health. 2020;2(4):e192–e200. doi: 10.1016/S2589-7500(20)30025-X - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
