

Colorectal cancer trends in Chile: A Latin-American country with marked socioeconomic inequities
- PMID: 36355864
- PMCID: PMC9648833
- DOI: 10.1371/journal.pone.0271929
Colorectal cancer trends in Chile: A Latin-American country with marked socioeconomic inequities
Abstract
Introduction: Colorectal cancer (CRC) is the third most frequent malignant disease in the world. In some countries with established screening programs, its incidence and mortality have decreased, and survival has improved.
Aims: To obtain reliable data about the epidemiology of CRC in Chile, we analyzed the trends in the last ten years and the influence of observable factors on survival, including a nationwide health program for CRC treatment access (GES program).
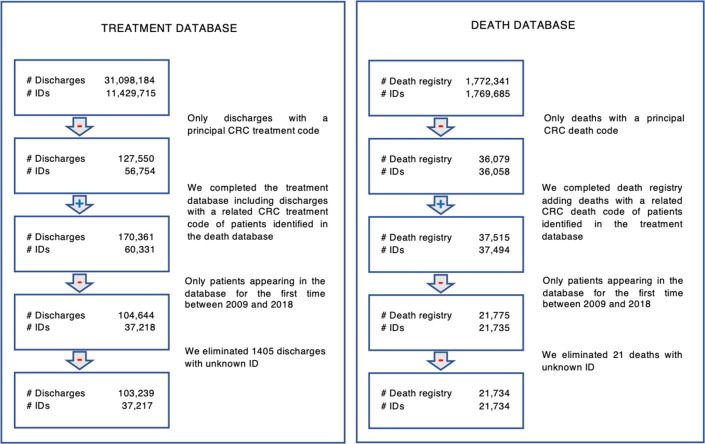
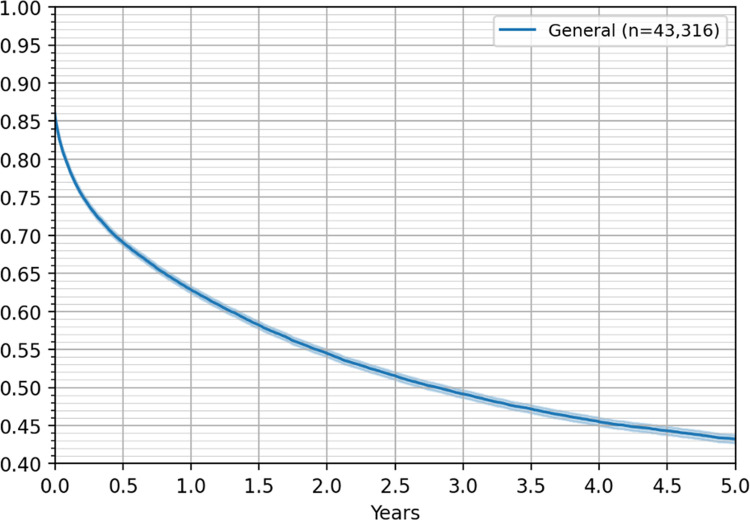
Methods: Publicly available data published by the Ministry of Health and National Institute of Statistics were used. Data were obtained from registries of mortality and hospital discharges, making follow-up of the individuals possible. Crude and age-standardized incidence and mortality rates were calculated, and individual survival was studied by constructing Kaplan-Meier curves. Finally, a Cox statistical model was established to estimate the impact of the observable factors.
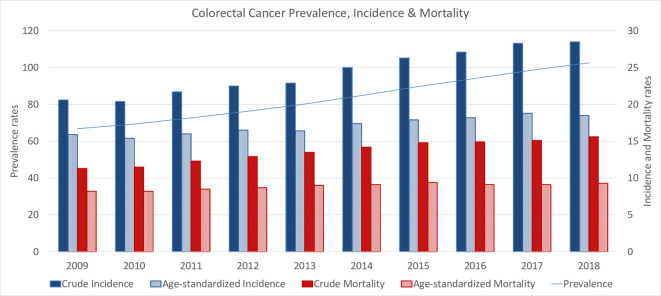
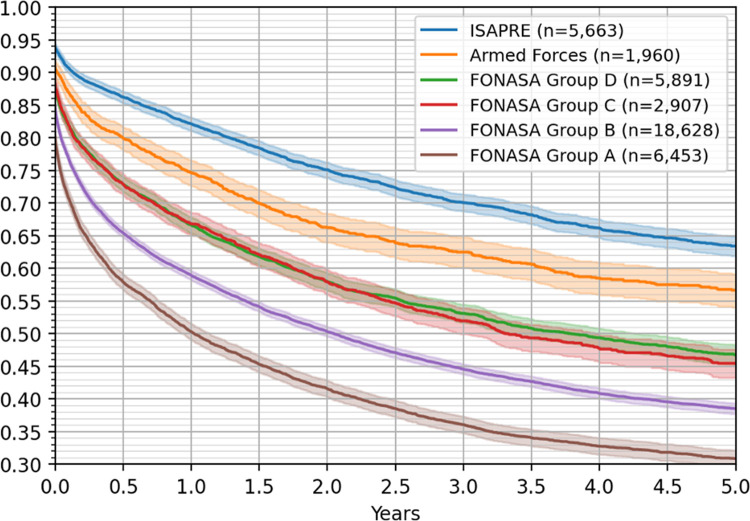
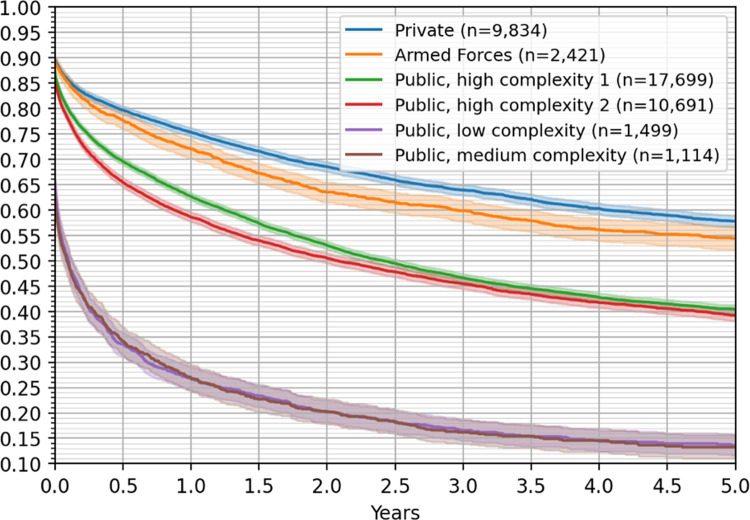
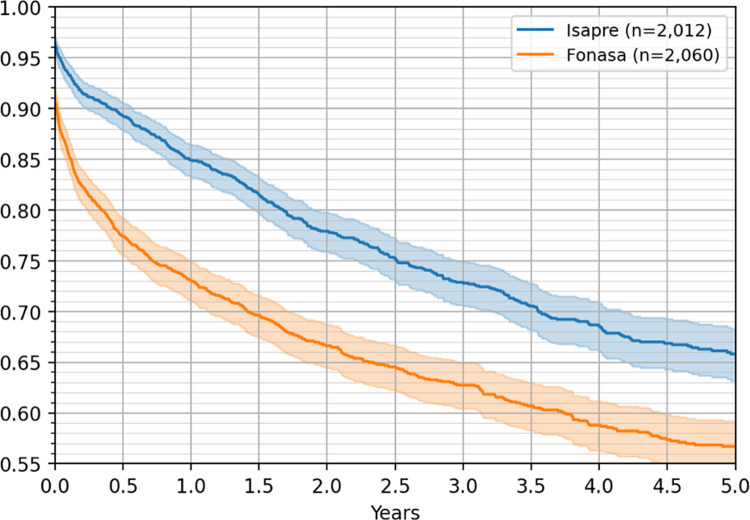
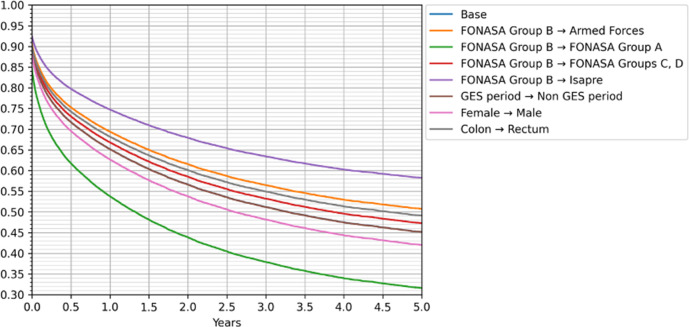
Results: We found 37,217 newly identified CRC patients between 2008 and 2019 in Chile, corresponding to 103,239 hospital discharges. In the same period, 24,217 people died of CRC. A nearly linear, steady increase in crude incidence, mortality and prevalence was observed. CRC incidence was the lowest in the North of the country, increasing toward the South and reaching a maximum value of 34.6/100,000 inhabitants/year in terms of crude incidence and 20.7/100,000 inhabitants/year in terms of crude mortality in the XII region in 2018. We found that older patients had lower survival rates, as well as men compared to women. Survival was significantly better for patients with private insurance than those under the public insurance system, and the treating hospital also played a significant role in the survival of patients. Patients in the capital region survived longer than those in almost every other part of the country. We found no significant effect on survival associated with the GES program.
Conclusions: We found important inequalities in the survival probabilities for CRC patients in Chile. Survival depends mainly on the type of insurance, access to more complex hospitals, and geographical location; all three factors correlated with socioeconomic status of the population. Our work emphasized the need to create specific programs addressing primary causes to decrease the differences in CRC survival.
Copyright: © 2022 Mondschein et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Lu B., Li N., Luo C., Cai J., Lu M., Zhang Y. and et al.., "Colorectal cancer incidence and mortality: the current status, temporal trends and their attributable risk factors in 60 countries in 2000–2019.," Chin Med J (Engl), pp. 134(16):1941–1951, 2021. doi: 10.1097/CM9.0000000000001619 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
