

Impact of Acute Exacerbation and Its Phenotypes on the Clinical Outcomes of Chronic Obstructive Pulmonary Disease in Hospitalized Patients: A Cross-Sectional Study
- PMID: 36355958
- PMCID: PMC9695923
- DOI: 10.3390/toxics10110667
Impact of Acute Exacerbation and Its Phenotypes on the Clinical Outcomes of Chronic Obstructive Pulmonary Disease in Hospitalized Patients: A Cross-Sectional Study
Abstract
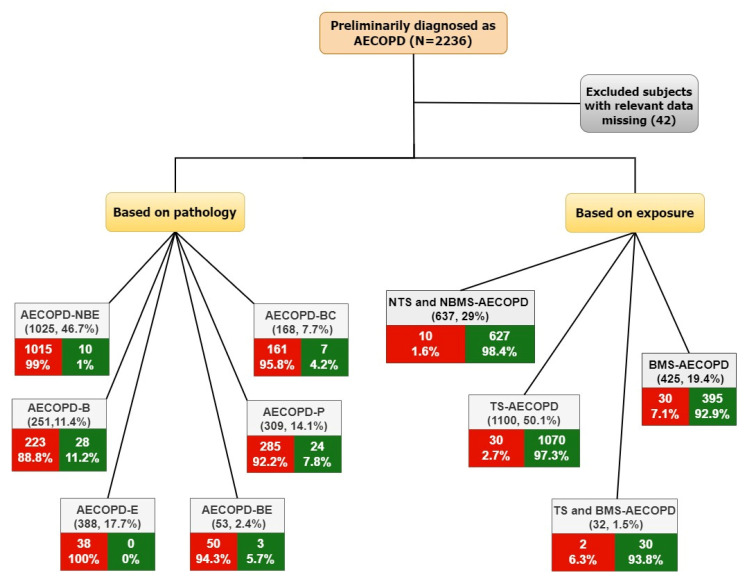
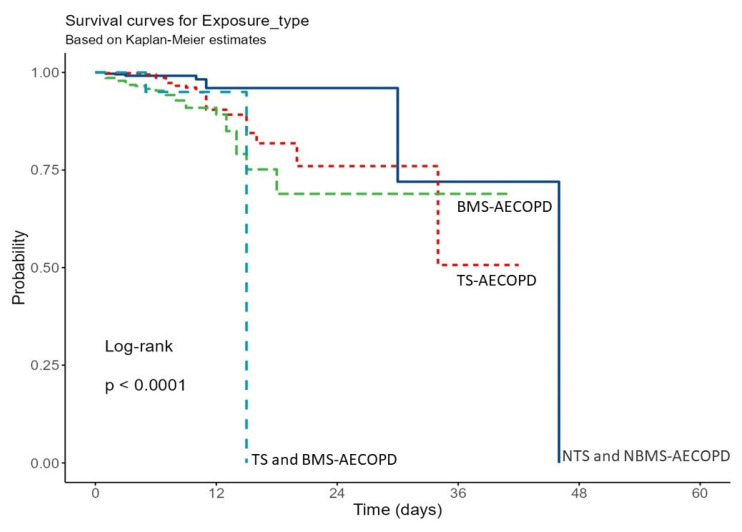
Acute exacerbations of COPD (AECOPD) are clinically significant events having therapeutic and prognostic consequences. However, there is a lot of variation in its clinical manifestations described by phenotypes. The phenotypes of AECOPD were categorized in this study based on pathology and exposure. In our cross-sectional study, conducted between 1 January 2016 to 31 December 2020, the patients were categorized into six groups based on pathology: non-bacterial and non-eosinophilic; bacterial; eosinophilic; bacterial infection with eosinophilia; pneumonia; and bronchiectasis. Further, four groups were classified based on exposure to tobacco smoke (TS), biomass smoke (BMS), both, or no exposure. Cox proportional-hazards regression analyses were performed to assess hazard ratios, and Kaplan-Meier analysis was performed to assess survival, which was then compared using the log-rank test. The odds ratio (OR) and independent predictors of ward admission type and length of hospital stay were assessed using binomial logistic regression analyses. Of the 2236 subjects, 2194 were selected. The median age of the cohort was 67.0 (60.0 to 74.0) and 75.2% were males. Mortality rates were higher in females than in males (6.2% vs. 2.3%). AECOPD-B (bacterial infection) subjects [HR 95% CI 6.42 (3.06-13.46)], followed by AECOPD-P (pneumonia) subjects [HR (95% CI: 4.33 (2.01-9.30)], were at higher mortality risk and had a more extended hospital stay (6.0 (4.0 to 9.5) days; 6.0 (4.0 to 10.0). Subjects with TS and BMS-AECOPD [HR 95% CI 7.24 (1.53-34.29)], followed by BMS-AECOPD [HR 95% CI 5.28 (2.46-11.35)], had higher mortality risk. Different phenotypes have different impacts on AECOPD clinical outcomes. A better understanding of AECOPD phenotypes could contribute to developing an algorithm for the precise management of different phenotypes.
Keywords: AECOPD; COPD; acute exacerbation; biomass; mortality; phenotype; tobacco.
Conflict of interest statement
The authors declare that this article’s content has no conflict of interest.
Figures

Similar articles
-
Effect of Community-Acquired Pneumonia on Acute Exacerbation of Chronic Obstructive Pulmonary Disease.COPD. 2021 Aug;18(4):417-424. doi: 10.1080/15412555.2021.1950664. Epub 2021 Jul 26. COPD. 2021. PMID: 34309464
-
Incidence and profile of severe exacerbations of chronic obstructive pulmonary disease due to biomass smoke or tobacco.Ann Thorac Med. 2022 Oct-Dec;17(4):193-198. doi: 10.4103/atm.atm_155_22. Epub 2022 Oct 7. Ann Thorac Med. 2022. PMID: 36387759 Free PMC article.
-
Early readmission and mortality in acute exacerbation of chronic obstructive pulmonary disease with community-acquired pneumonia.Chron Respir Dis. 2019 Jan-Dec;16:1479972318809480. doi: 10.1177/1479972318809480. Chron Respir Dis. 2019. PMID: 30428701 Free PMC article.
-
In-hospital antibiotic use for severe chronic obstructive pulmonary disease exacerbations: a retrospective observational study.BMC Pulm Med. 2023 Apr 25;23(1):138. doi: 10.1186/s12890-023-02426-3. BMC Pulm Med. 2023. PMID: 37098509 Free PMC article.
-
Etiology and epidemiology of acute exacerbations of chronic obstructive pulmonary disease in Eastern Nepal: a narrative review.Ann Med Surg (Lond). 2024 Aug 30;86(10):5995-5998. doi: 10.1097/MS9.0000000000002520. eCollection 2024 Oct. Ann Med Surg (Lond). 2024. PMID: 39359792 Free PMC article. Review.
Cited by
-
Effect of pneumonia on the outcomes of acute exacerbation of chronic obstructive pulmonary disease: a systematic review and meta-analysis.BMC Pulm Med. 2024 Oct 9;24(1):496. doi: 10.1186/s12890-024-03305-1. BMC Pulm Med. 2024. PMID: 39385140 Free PMC article.
-
Factors Affecting Survival in Severe and Very Severe COPD after Admission in ICUs of Tertiary Care Centers of India (FAST COPD): Study Protocol for a Multicentric Cohort Study.Indian J Crit Care Med. 2024 Jun;28(6):552-560. doi: 10.5005/jp-journals-10071-24728. Indian J Crit Care Med. 2024. PMID: 39130380 Free PMC article.
-
Re-exacerbation within 30 days of discharge is associated with poor prognosis in the following year among patients hospitalised with exacerbation of chronic obstructive pulmonary disease: a clinical cohort study.BMJ Open Respir Res. 2023 Aug;10(1):e001759. doi: 10.1136/bmjresp-2023-001759. BMJ Open Respir Res. 2023. PMID: 37640511 Free PMC article.
-
Clinical Characteristics and Outcomes of Hospitalized AECOPDs Secondary to SARS-CoV-2 versus Other Respiratory Viruses.Int J Chron Obstruct Pulmon Dis. 2024 Nov 14;19:2421-2430. doi: 10.2147/COPD.S479968. eCollection 2024. Int J Chron Obstruct Pulmon Dis. 2024. PMID: 39559372 Free PMC article.
-
Unmasking the Silent Threat: Periodontal Health's Impact on COPD Severity and Hospitalization.J Pers Med. 2023 Dec 15;13(12):1714. doi: 10.3390/jpm13121714. J Pers Med. 2023. PMID: 38138940 Free PMC article.
References
-
- Pauwels R.A., Buist A.S., Calverley P.M.A., Jenkins C.R., Hurd S.S. GOLD Scientific Committee Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease: NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop Summary. Am. J. Respir. Crit. Care Med. 2001;163:1256–1276. doi: 10.1164/ajrccm.163.5.2101039. - DOI - PubMed
-
- GOLD Report 2022. 2022. [(accessed on 1 November 2022)]. pp. 1–165. Available online: https://goldcopd.org/2022-gold-reports-2/
-
- Grigsby M., Siddharthan T., Chowdhury M., Siddiquee A., Rubinstein A., Sobrino E., Miranda J.J., Bernabe-Ortiz A., Alam D., Checkley W. Socioeconomic Status and COPD among Low- and Middle-Income Countries. Int. J. Chron. Obstruct. Pulmon. Dis. 2016;11:2497–2507. doi: 10.2147/COPD.S111145. - DOI - PMC - PubMed
-
- Buist A.S., McBurnie M.A., Vollmer W.M., Gillespie S., Burney P., Mannino D.M., Menezes A.M., Sullivan S.D., Lee T.A., Weiss K.B., et al. International Variation in the Prevalence of COPD (The BOLD Study): A Population-Based Prevalence Study. Lancet. 2007;370:741–750. doi: 10.1016/S0140-6736(07)61377-4. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
