

Changes in anticancer treatment plans in patients with solid cancer hospitalized with COVID-19: analysis of the nationwide BSMO-COVID registry providing lessons for the future
- PMID: 36356416
- PMCID: PMC9639795
- DOI: 10.1016/j.esmoop.2022.100610
Changes in anticancer treatment plans in patients with solid cancer hospitalized with COVID-19: analysis of the nationwide BSMO-COVID registry providing lessons for the future
Abstract
Background: Solid cancer is an independent prognostic factor for poor outcome with COVID-19. As guidelines for patient management in that setting depend on retrospective efforts, we here present the first analyses of a nationwide database of patients with cancer hospitalized with COVID-19 in Belgium, with a focus on changes in anticancer treatment plans at the time of SARS-CoV-2 infection.
Methods: Nineteen Belgian hospitals identified all patients with a history of solid cancer hospitalized with COVID-19 between March 2020 and February 2021. Demographic, cancer-specific and COVID-specific data were pseudonymously entered into a central Belgian Society of Medical Oncology (BSMO)-COVID database. The association between survival and primary cancer type was analyzed through multivariate multinomial logistic regression. Group comparisons for categorical variables were carried out through a Chi-square test.
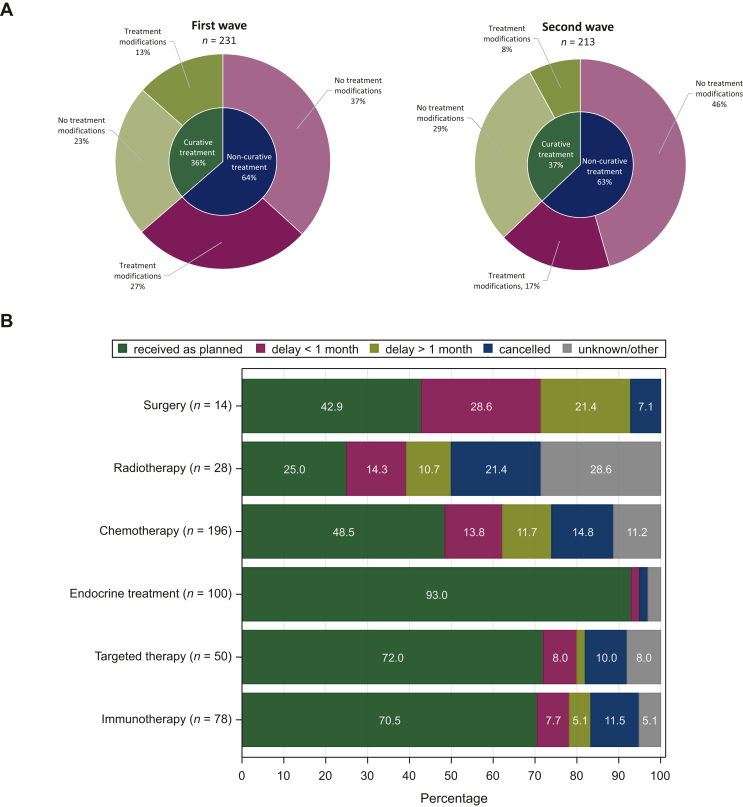
Results: A total of 928 patients were registered in the database; most of them were aged ≥70 years (61.0%) and with poor performance scores [57.2% Eastern Cooperative Oncology Group (ECOG) ≥2]. Thirty-day COVID-related mortality was 19.8%. In multivariate analysis, a trend was seen for higher mortality in patients with lung cancer (27.6% versus 20.8%, P = 0.062) and lower mortality for patients with breast cancer (13.0% versus 23.3%, P = 0.052) compared with other tumour types. Non-curative treatment was associated with higher 30-day COVID-related mortality rates compared with curative or no active treatment (25.8% versus 14.3% versus 21.9%, respectively, P < 0.001). In 33% of patients under active treatment, the therapeutic plan was changed due to COVID-19 diagnosis, most frequently involving delays/interruptions in systemic treatments (18.6%). Thirty-day COVID-related mortality was not significantly different between patients with and without treatment modifications (21.4% versus 20.5%).
Conclusion: Interruption in anticancer treatments at the time of SARS-CoV-2 infection was not associated with a reduction in COVID-related mortality in our cohort of patients with solid cancer, highlighting that treatment continuation should be strived for, especially in the curative setting.
Keywords: COVID-19; cancer; prognosis; solid tumours; treatment changes.
Copyright © 2022 The Authors. Published by Elsevier Ltd.. All rights reserved.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
