

Non-viral precision T cell receptor replacement for personalized cell therapy
- PMID: 36356599
- PMCID: PMC9768791
- DOI: 10.1038/s41586-022-05531-1
Non-viral precision T cell receptor replacement for personalized cell therapy
Abstract
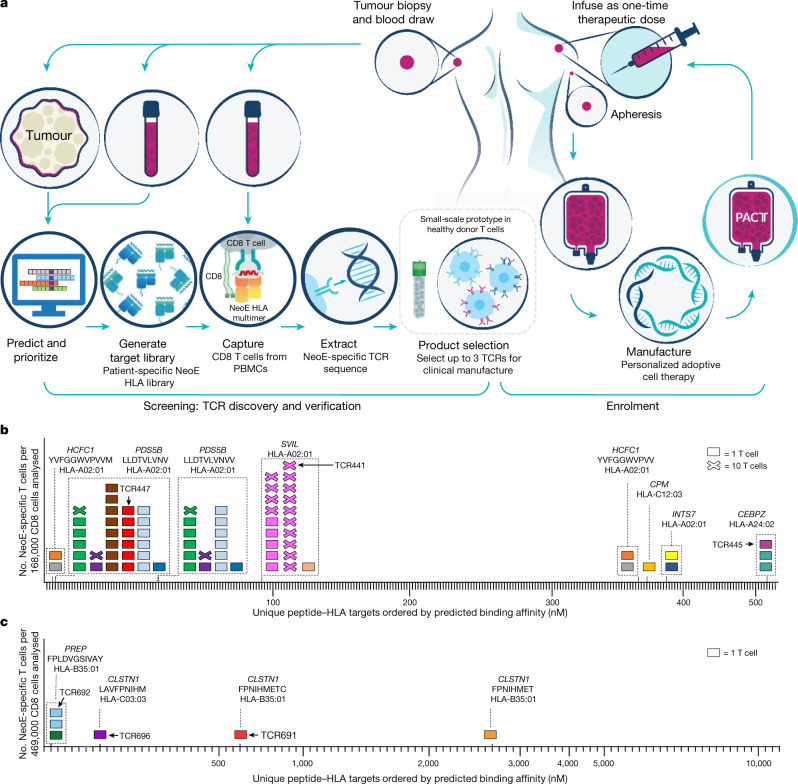
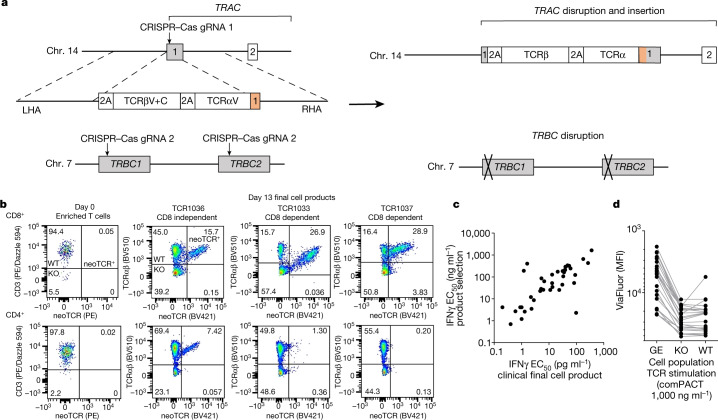
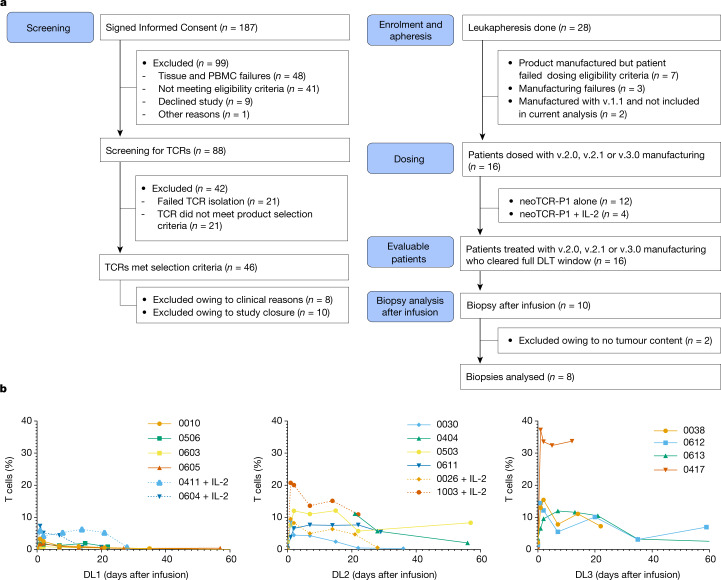
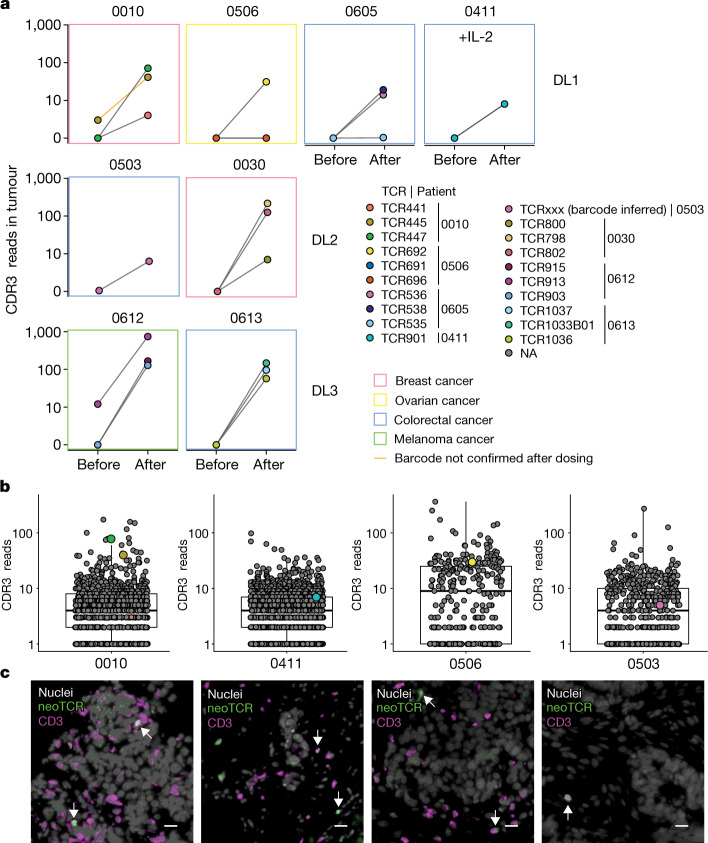
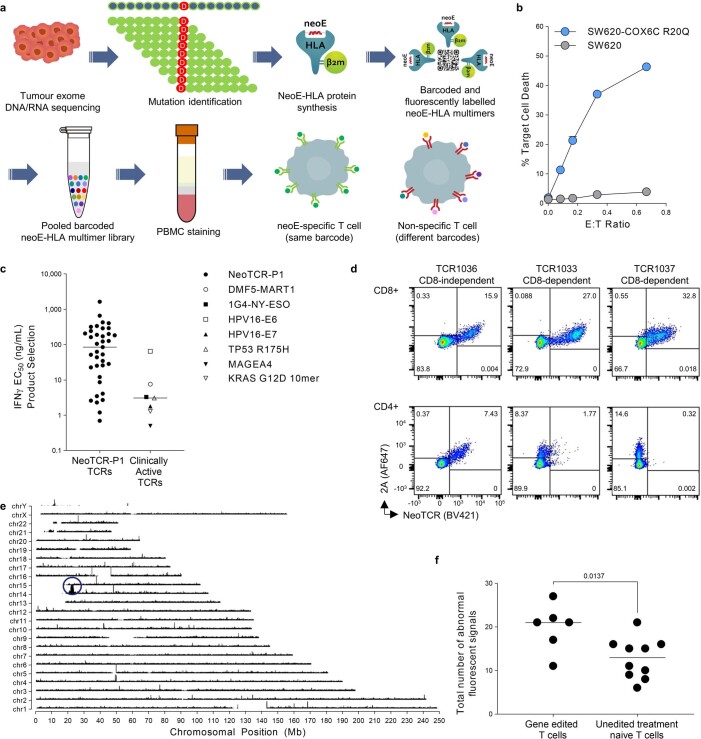
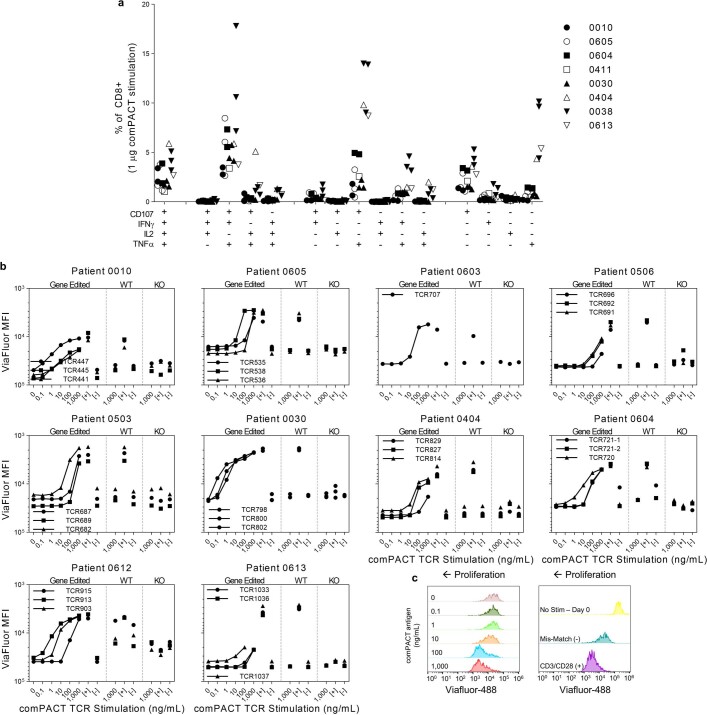
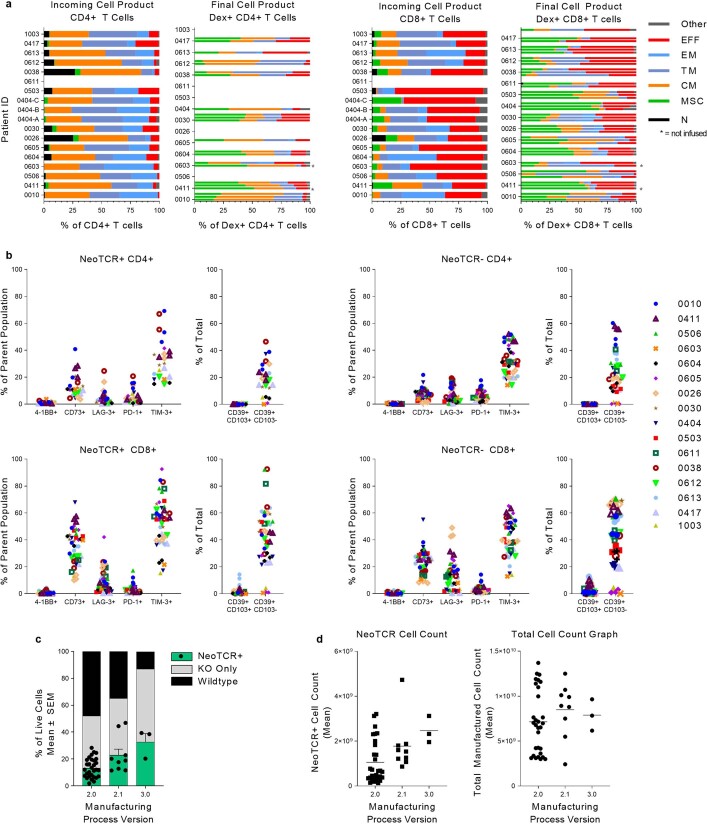
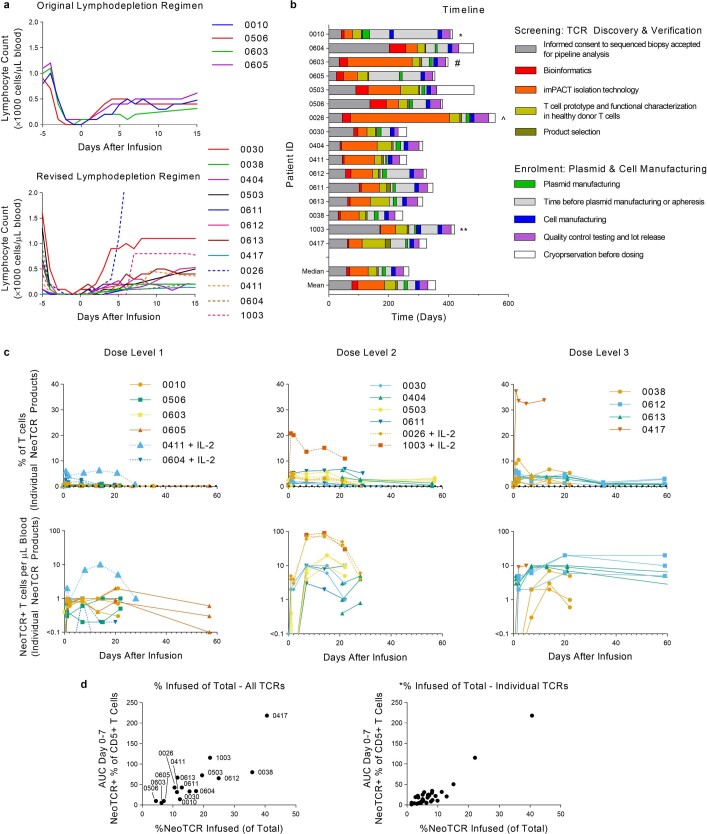
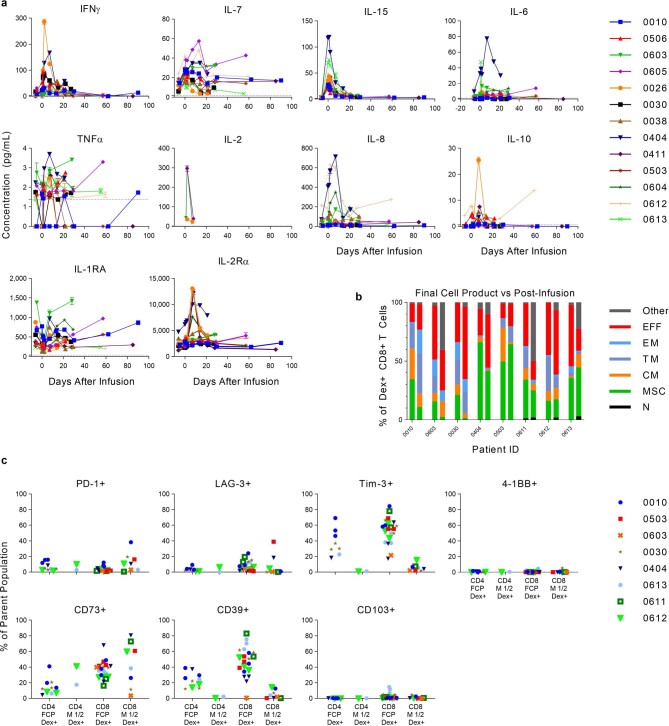
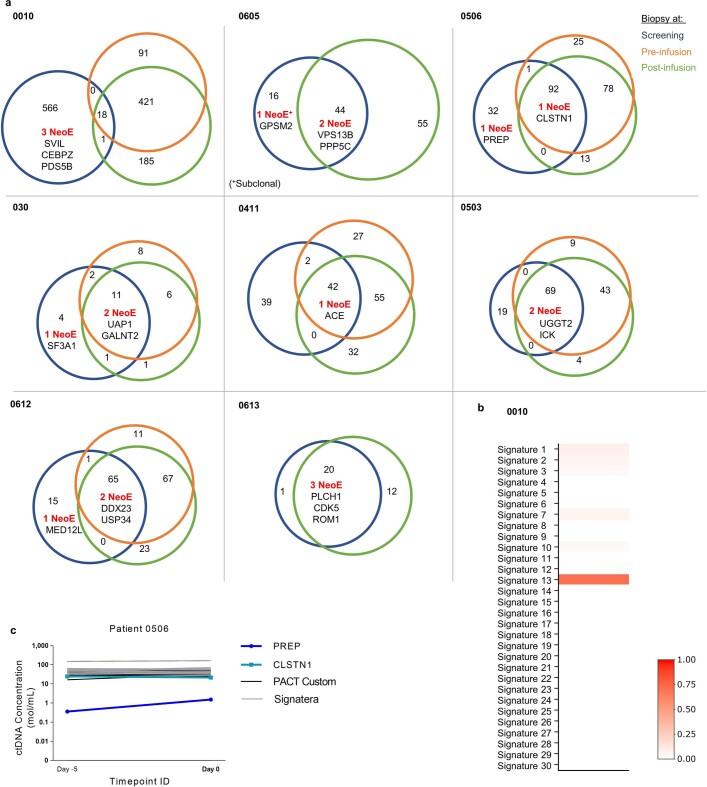
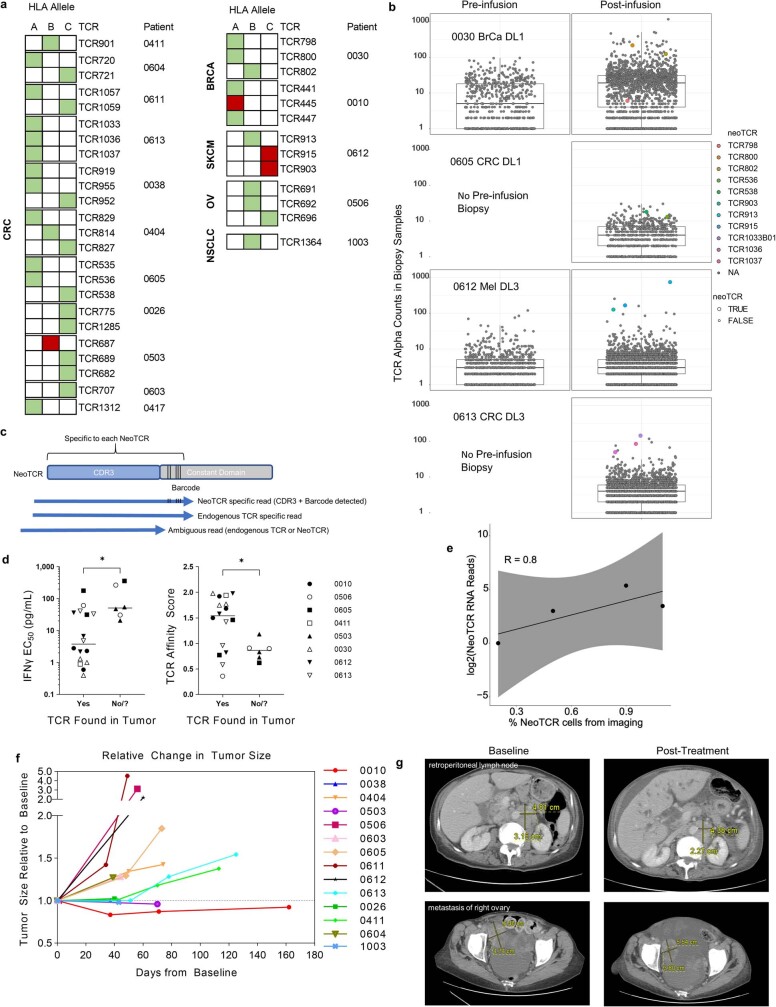
T cell receptors (TCRs) enable T cells to specifically recognize mutations in cancer cells1-3. Here we developed a clinical-grade approach based on CRISPR-Cas9 non-viral precision genome-editing to simultaneously knockout the two endogenous TCR genes TRAC (which encodes TCRα) and TRBC (which encodes TCRβ). We also inserted into the TRAC locus two chains of a neoantigen-specific TCR (neoTCR) isolated from circulating T cells of patients. The neoTCRs were isolated using a personalized library of soluble predicted neoantigen-HLA capture reagents. Sixteen patients with different refractory solid cancers received up to three distinct neoTCR transgenic cell products. Each product expressed a patient-specific neoTCR and was administered in a cell-dose-escalation, first-in-human phase I clinical trial ( NCT03970382 ). One patient had grade 1 cytokine release syndrome and one patient had grade 3 encephalitis. All participants had the expected side effects from the lymphodepleting chemotherapy. Five patients had stable disease and the other eleven had disease progression as the best response on the therapy. neoTCR transgenic T cells were detected in tumour biopsy samples after infusion at frequencies higher than the native TCRs before infusion. This study demonstrates the feasibility of isolating and cloning multiple TCRs that recognize mutational neoantigens. Moreover, simultaneous knockout of the endogenous TCR and knock-in of neoTCRs using single-step, non-viral precision genome-editing are achieved. The manufacture of neoTCR engineered T cells at clinical grade, the safety of infusing up to three gene-edited neoTCR T cell products and the ability of the transgenic T cells to traffic to the tumours of patients are also demonstrated.
© 2022. The Author(s).
Conflict of interest statement
S.P.F., K.J., T.H., Z.P., E.S., Y.M., W.L., S.P., C.L.W., B.Y., O.D., K.H., B.S., A.C., M.T.B., I.M., W.W., M.K., S.G., E.H., A.H., D. An, A.J.L., B.B.Q., C.S., D. Anaya, L.S., E.Y.-H.H., V.M., J.M., L.D., B.P., R.M., M.C.Y., R.F., A.S., T.S.-S., A.F., A.V.R. and S.J.M. were employees of PACT Pharma during the conduct of this work. S.P., M.T.B., D.B., J.R.H. and A.R. are scientific co-founders of PACT Pharma. K.M.C. has received consulting fees from PACT Pharma and Tango Therapeutics and is a shareholder in Geneoscopy. D.Y.O. has received research support from Merck, PACT Pharma, the Parker Institute for Cancer Immunotherapy, Poseida Therapeutics, TCR2 Therapeutics, Roche/Genentech and Nutcracker Therapeutics. B.C. has advisory roles with the following companies: Iovance Biotherapeutics, IDEAYA Biosciences, Sanofi, OncoSec, Nektar, Genentech, Novartis and Instil Bio. D.Y.O. has also received research funding from the following companies: Iovance Biotherapeutics, Bristol-Myers Squibb, Macrogenics, Daiichi Sankyo, Merck, Karyopharm Therapeutics, Infinity Pharmaceuticals, Advenchen Laboratories, Idera, Neon Therapeutics, Xencor, Compugen, PACT Pharma, RAPT Therapeutics, Immunocore, Lilly, IDEAYA Biosciences, Tolero Pharmaceuticals, Ascentage Pharma, Novartis, Atreca, Replimune, Instil Bio, Trisalus and Kinnate. J.A.S. reports honorarium from Iovance, Apixogen, Jazz Pharm, and research with BMS, PACT Pharma and Corvus. A.J.S. reports consulting or advising roles to J&J, KSQ Therapeutics, BMS, Enara Bio, Perceptive Advisors, Heat Biologics and Iovance Biotherapeutics. Research funding: GSK (Inst), PACT pharma (Inst), Iovance Biotherapeutics (Inst), Achilles therapeutics (Inst), Merck (Inst), BMS (Inst), Harpoon Therapeutics (Inst). A.R. has received honoraria from consulting with Amgen, CStone, Merck, and Vedanta, is or has been a member of the scientific advisory board and holds stock in Advaxis, Appia, Apricity, Arcus, Compugen, CytomX, Highlight, ImaginAb, ImmPact, ImmuneSensor, Inspirna, Isoplexis, Kite-Gilead, Lutris, MapKure, Merus, PACT Pharma, Pluto, RAPT, Synthekine and Tango, has received research funding from Agilent and from Bristol-Myers Squibb through Stand Up to Cancer (SU2C), and patent royalties from Arsenal Bio. D.A.B., A.H.C.N., Y.L., M.A., Y.Y. and S.M.L. report no conflicts of interest for this work.
Figures
Comment in
-
CRISPR cancer trial success paves the way for personalized treatments.Nature. 2022 Nov;611(7936):433-434. doi: 10.1038/d41586-022-03676-7. Nature. 2022. PMID: 36357583 No abstract available.
-
TCR-engineered T cells get personal.Nat Rev Drug Discov. 2023 Jan;22(1):18. doi: 10.1038/d41573-022-00208-w. Nat Rev Drug Discov. 2023. PMID: 36460864 No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
