

Treatment pattern trends of medications for type 2 diabetes in British Columbia, Canada
- PMID: 36356988
- PMCID: PMC9660664
- DOI: 10.1136/bmjdrc-2022-002995
Treatment pattern trends of medications for type 2 diabetes in British Columbia, Canada
Abstract
Introduction: Several new oral drug classes for type 2 diabetes (T2DM) have been introduced in the last 20 years accompanied by developments in clinical evidence and guidelines. The uptake of new therapies and contemporary use of blood glucose-lowering drugs has not been closely examined in Canada. The objective of this project was to describe these treatment patterns and relate them to changes in provincial practice guidelines.
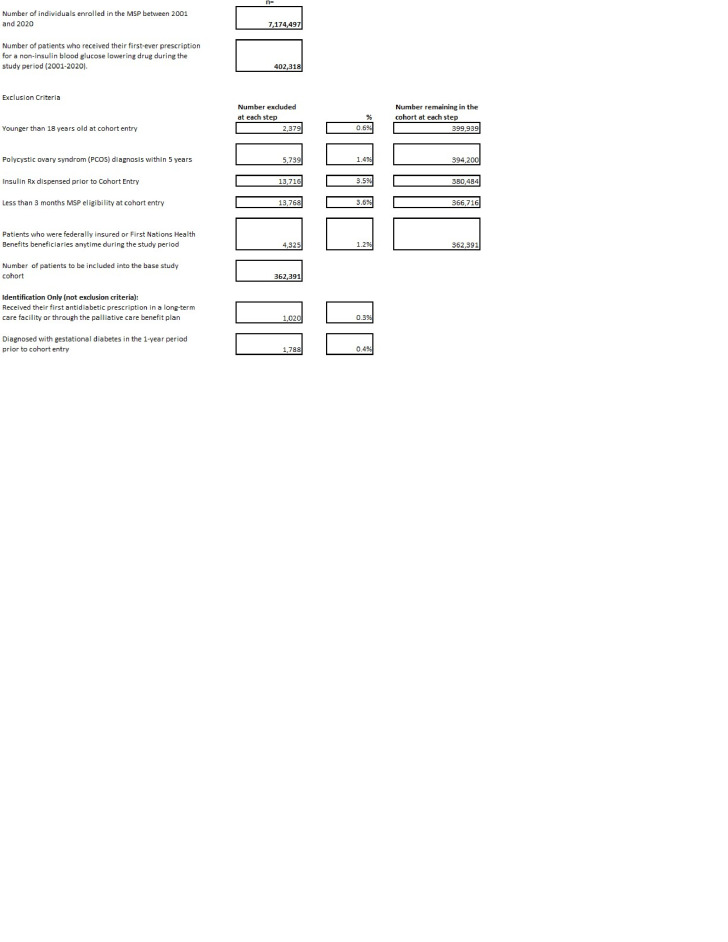
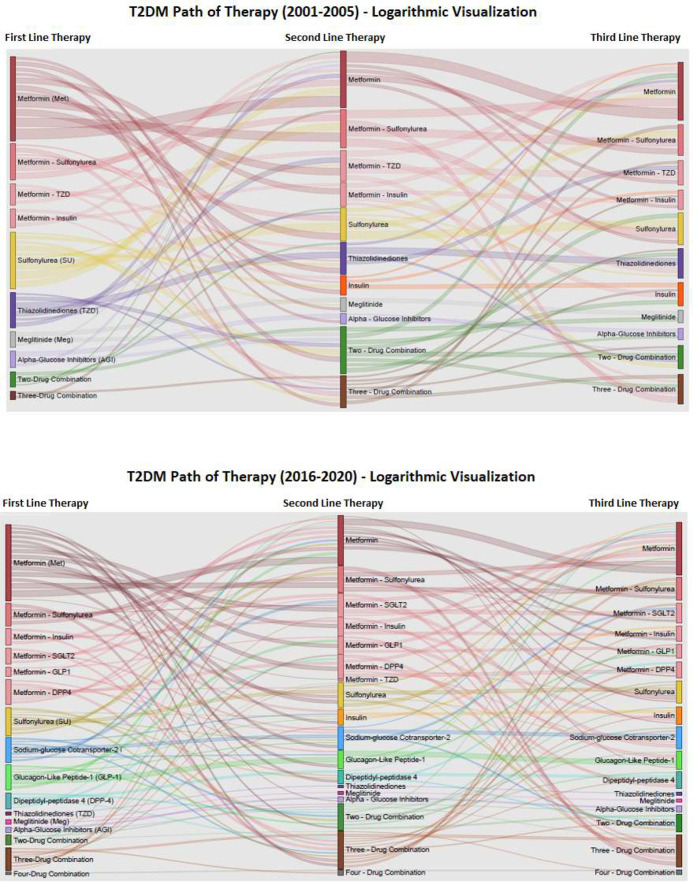
Research design and methods: We conducted a longitudinal drug utilization study among persons with T2DM aged ≥18 years from 2001 to 2020 in British Columbia (BC), Canada. We used dispensing data from community pharmacies with linkable physician billing and hospital admission records. Laboratory results were available from 2011 onwards. We identified incident users of blood glucose-lowering drugs, then determined sequence patterns of medications dispensed, with stratification by age group, and subgroup analysis for patients with a history of cardiovascular disease.
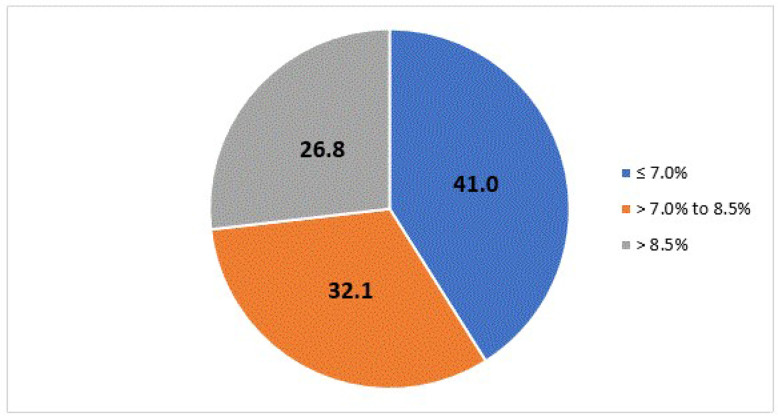
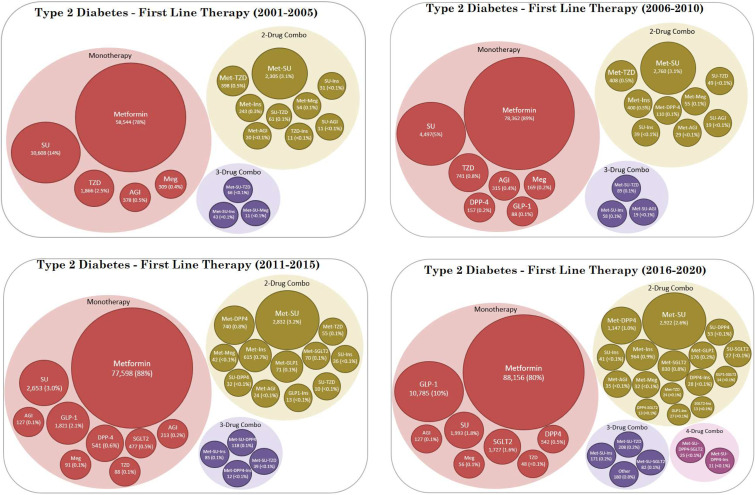
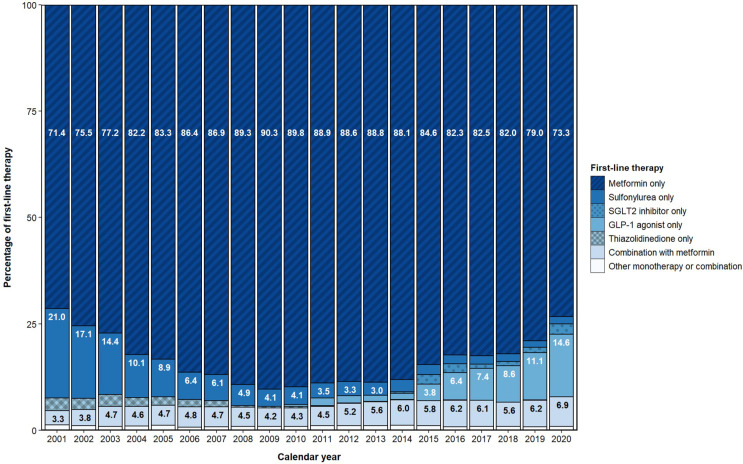
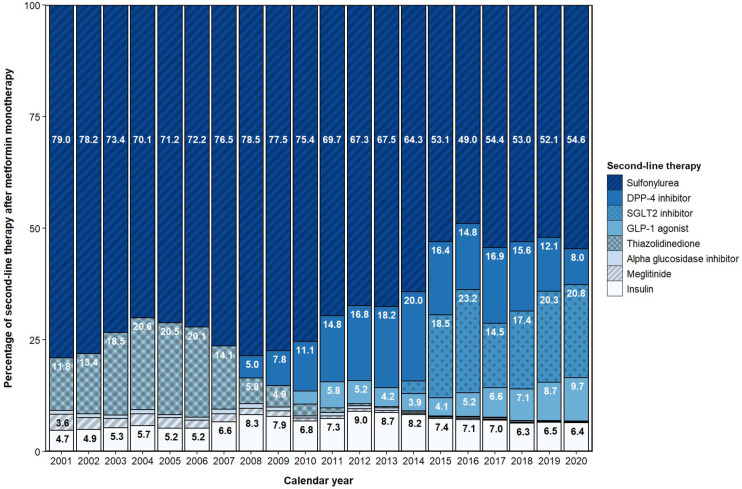
Results: Among a cohort of 362 391 patients (mean age 57.7 years old, 53.5% male) treated for non-insulin-dependent diabetes, the proportion who received metformin monotherapy as first-line treatment reached a maximum of 90% in 2009, decreasing to 73% in 2020. The proportion of patients starting two-drug combinations nearly doubled from 3.3% to 6.4%. Sulfonylureas were the preferred class of second-line agents over the course of the study period. In 2020, sodium-glucose cotransporter type 2 inhibitors and glucagon-like peptide-1 receptor agonists accounted for 21% and 10% of second-line prescribing, respectively. For patients with baseline glycated hemoglobin (A1C) results prior to initiating diabetic treatment, 41% had a value ≤7.0% and 27% had a value over 8.5%.
Conclusions: Oral diabetic medication patterns have changed significantly over the last 20 years in BC, primarily in terms of medications used as second-line therapy. Over 40% of patients with available laboratory results initiated T2DM treatment with an A1C value ≤7.0%, with the average A1C value trending lower over the last decade.
Keywords: diabetes mellitus, type 2; drug utilization; health services research; practice guideline.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Factors Associated with Type 2 Diabetes Mellitus Treatment Choice Across Four European Countries.Clin Ther. 2017 Nov;39(11):2296-2310.e14. doi: 10.1016/j.clinthera.2017.09.016. Epub 2017 Nov 4. Clin Ther. 2017. PMID: 29108837
-
Prescribing Paradigm Shift? Applying the 2019 European Society of Cardiology-Led Guidelines on Diabetes, Prediabetes, and Cardiovascular Disease to Assess Eligibility for Sodium-Glucose Cotransporter 2 Inhibitors or Glucagon-Like Peptide 1 Receptor Agonists as First-Line Monotherapy (or Add-on to Metformin Monotherapy) in Type 2 Diabetes in Scotland.Diabetes Care. 2020 Sep;43(9):2034-2041. doi: 10.2337/dc20-0120. Epub 2020 Jun 24. Diabetes Care. 2020. PMID: 32581068
-
Changes in the Prescription of Glucose-Lowering Medications in Patients With Type 2 Diabetes Mellitus After a Cardiovascular Event: A Call to Action From the DATAFILE Study.J Am Heart Assoc. 2019 Jul 16;8(14):e012244. doi: 10.1161/JAHA.119.012244. Epub 2019 Jul 4. J Am Heart Assoc. 2019. PMID: 31269877 Free PMC article.
-
Clinical Review: Safety and Efficacy Comparison between Sulfonylureas and Dipeptidyl Peptidase-4 Inhibitors as Second-Line Therapies in Type 2 Diabetes Mellitus.Curr Pharm Des. 2020;26(34):4315-4322. doi: 10.2174/1381612826666200408095310. Curr Pharm Des. 2020. PMID: 32268860
-
Dipeptidyl peptidase-4 inhibitors for treatment of type 2 diabetes mellitus in the clinical setting: systematic review and meta-analysis.BMJ. 2012 Mar 12;344:e1369. doi: 10.1136/bmj.e1369. BMJ. 2012. PMID: 22411919
Cited by
-
Prescribing patterns of glucagon-like peptide-1 receptor agonists in the Swedish capital region-a register-based cross-sectional study.Eur J Clin Pharmacol. 2025 May;81(5):739-753. doi: 10.1007/s00228-025-03823-9. Epub 2025 Mar 13. Eur J Clin Pharmacol. 2025. PMID: 40074942 Free PMC article.
-
Comparative Effectiveness of Sodium-Glucose Cotransporter-2 Inhibitors for Recurrent Gout Flares and Gout-Primary Emergency Department Visits and Hospitalizations : A General Population Cohort Study.Ann Intern Med. 2023 Aug;176(8):1067-1080. doi: 10.7326/M23-0724. Epub 2023 Jul 25. Ann Intern Med. 2023. PMID: 37487215 Free PMC article.
-
Trends in diabetes medication prescribing from 2018 to 2021: A cross-sectional analysis.PLoS One. 2024 Aug 15;19(8):e0307451. doi: 10.1371/journal.pone.0307451. eCollection 2024. PLoS One. 2024. PMID: 39146274 Free PMC article.
-
Psoriasis Risk Is Lower in Type 2 Diabetes Patients Using Dipeptidyl Peptidase-4 Inhibitors or Thiazolidinediones Compared to Sulfonylureas.Clin Transl Sci. 2025 Mar;18(3):e70177. doi: 10.1111/cts.70177. Clin Transl Sci. 2025. PMID: 40075548 Free PMC article.
-
The 10 top prescribed medicines in Germany from 1985 to 2022: pharmacological analysis.Naunyn Schmiedebergs Arch Pharmacol. 2025 May;398(5):5509-5529. doi: 10.1007/s00210-024-03615-5. Epub 2024 Nov 21. Naunyn Schmiedebergs Arch Pharmacol. 2025. PMID: 39570381 Free PMC article.
References
-
- Ledger S. Diabetes mellitus Canadian clinical practice guidelines update. Cannt J 2004;14:38–44. quiz 44-5. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical