

Body weight-supported gait training for patients with spinal cord injury: a network meta-analysis of randomised controlled trials
- PMID: 36357483
- PMCID: PMC9649733
- DOI: 10.1038/s41598-022-23873-8
Body weight-supported gait training for patients with spinal cord injury: a network meta-analysis of randomised controlled trials
Abstract
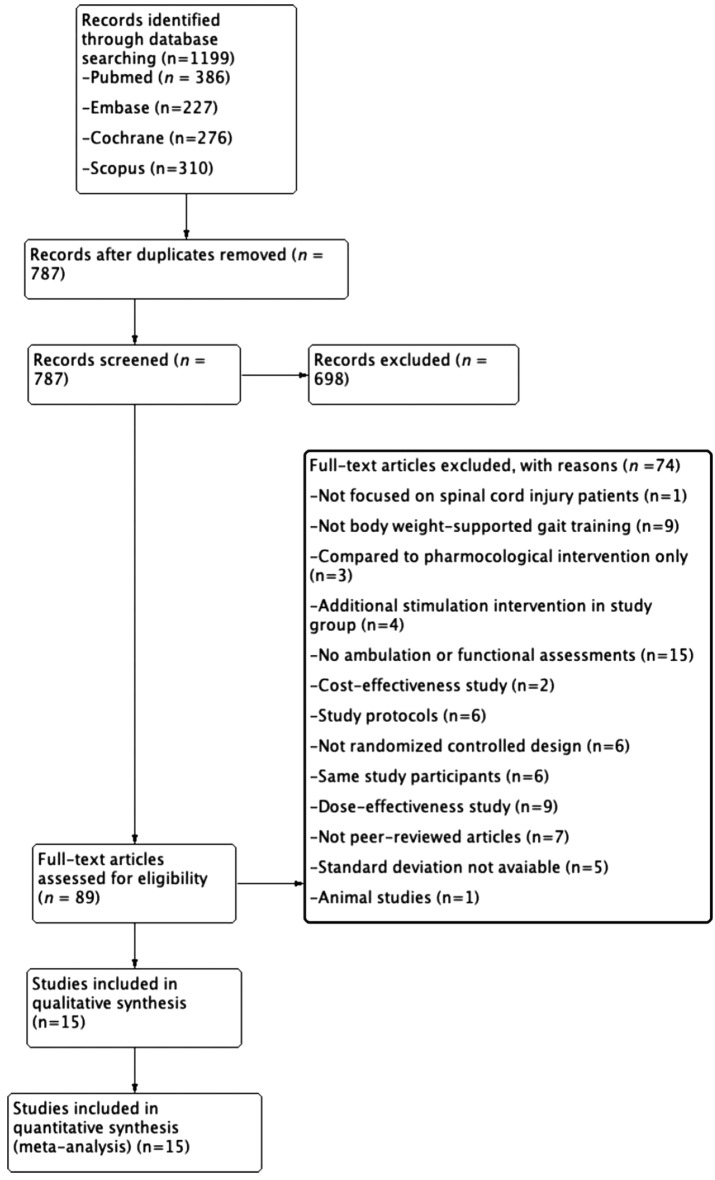
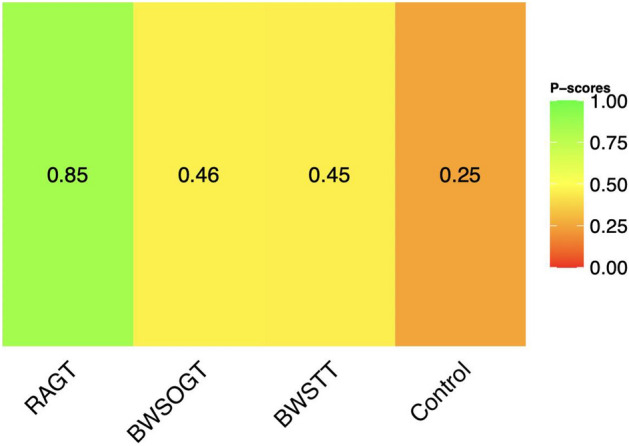
Different body weight-supported gait-training strategies are available for improving ambulation in individuals with spinal cord injury (SCI). These include body weight-supported overground training (BWSOGT), body weight-supported treadmill training (BWSTT), and robot-assisted gait training (RAGT). We conducted a network meta-analysis of randomised controlled trials (RCTs) to assess the effect and priority of each training protocol. We searched the PubMed, Cochrane Library, Scopus, and Embase databases from inception to 6 August 2022. The eligibility criteria were as follows: (1) being RCTs, (2) recruiting participants with SCI diagnosis and requiring gait training, (3) comparing different body weight-supported gait training strategies, and (4) involving ambulatory assessments. We conducted a network meta-analysis to compare different training strategies using the standard mean difference and its 95% credible interval. To rank the efficacy of training strategies, we used the P score as an indicator. Inconsistency in network meta-analysis was evaluated using loop-specific heterogeneity. We included 15 RCTs in this analysis. RAGT was had significantly more favourable performance than had the control intervention. The ranking probabilities indicated that the most effective approach was RAGT, followed by BWSOGT, BWSTT, and the control intervention. No significant inconsistency was noted between the results of the direct and indirect comparisons.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures




Similar articles
-
Which gait training intervention can most effectively improve gait ability in patients with cerebral palsy? A systematic review and network meta-analysis.Front Neurol. 2023 Jan 10;13:1005485. doi: 10.3389/fneur.2022.1005485. eCollection 2022. Front Neurol. 2023. PMID: 36703638 Free PMC article.
-
The effects of robot assisted gait training on temporal-spatial characteristics of people with spinal cord injuries: A systematic review.J Spinal Cord Med. 2018 Sep;41(5):529-543. doi: 10.1080/10790268.2018.1426236. Epub 2018 Feb 5. J Spinal Cord Med. 2018. PMID: 29400988 Free PMC article.
-
Effects of Robot-Assisted Gait Training in Individuals with Spinal Cord Injury: A Meta-analysis.Biomed Res Int. 2020 Mar 21;2020:2102785. doi: 10.1155/2020/2102785. eCollection 2020. Biomed Res Int. 2020. PMID: 32280681 Free PMC article. Review.
-
Effects of robot-assisted gait training on cardiopulmonary function and lower extremity strength in individuals with spinal cord injury: A systematic review and meta-analysis.J Spinal Cord Med. 2024 Jan;47(1):6-14. doi: 10.1080/10790268.2023.2188392. Epub 2023 Mar 27. J Spinal Cord Med. 2024. PMID: 36972206 Free PMC article.
-
Effect of robotic-assisted gait training on gait and motor function in spinal cord injury: a protocol of a systematic review with meta-analysis.BMJ Open. 2023 Sep 22;13(9):e070675. doi: 10.1136/bmjopen-2022-070675. BMJ Open. 2023. PMID: 37739462 Free PMC article.
Cited by
-
Non-invasive cerebral and spinal cord stimulation for motor and gait recovery in incomplete spinal cord injury: systematic review and meta-analysis.J Neuroeng Rehabil. 2025 Mar 7;22(1):53. doi: 10.1186/s12984-025-01557-4. J Neuroeng Rehabil. 2025. PMID: 40050875 Free PMC article.
-
Physiotherapists' User Acceptance of a Lower Limb Robotic Exoskeleton in Specialized Rehabilitation: Qualitative Exploratory Study.JMIR Rehabil Assist Technol. 2025 Apr 16;12:e68233. doi: 10.2196/68233. JMIR Rehabil Assist Technol. 2025. PMID: 40238235 Free PMC article.
-
Robot-assisted gait training in patients with various neurological diseases: A mixed methods feasibility study.PLoS One. 2024 Aug 27;19(8):e0307434. doi: 10.1371/journal.pone.0307434. eCollection 2024. PLoS One. 2024. PMID: 39190743 Free PMC article.
-
Rehabilitation to Improve Outcomes after Cervical Spine Surgery: Narrative Review.J Clin Med. 2024 Sep 10;13(18):5363. doi: 10.3390/jcm13185363. J Clin Med. 2024. PMID: 39336849 Free PMC article. Review.
-
The effect of robot-assisted gait training for patients with spinal cord injury: a systematic review and meta-analysis.Front Neurosci. 2023 Aug 22;17:1252651. doi: 10.3389/fnins.2023.1252651. eCollection 2023. Front Neurosci. 2023. PMID: 37680972 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
