

Temporary mechanical circulatory support devices: practical considerations for all stakeholders
- PMID: 36357709
- PMCID: PMC9649020
- DOI: 10.1038/s41569-022-00796-5
Temporary mechanical circulatory support devices: practical considerations for all stakeholders
Abstract
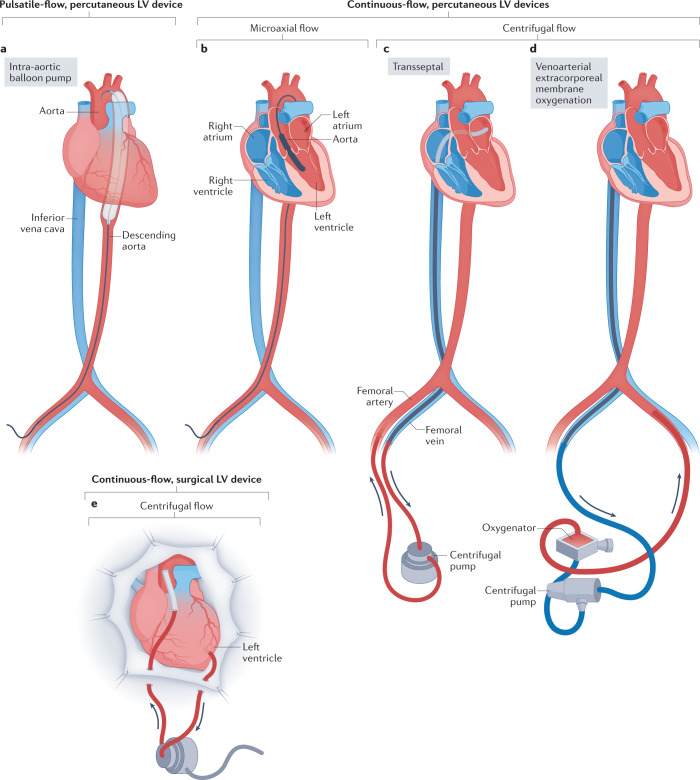
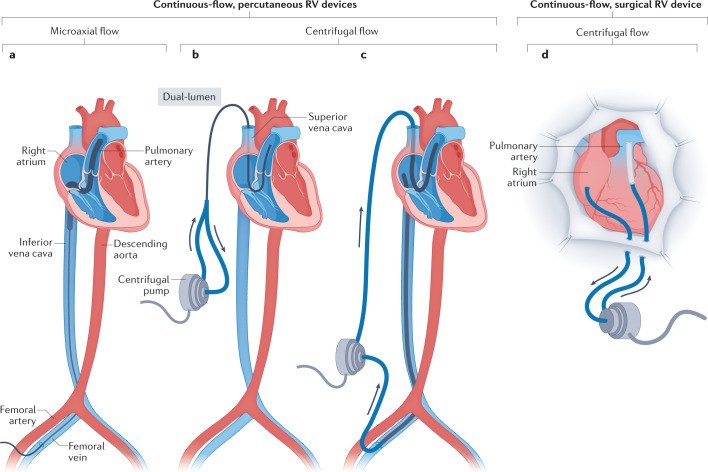
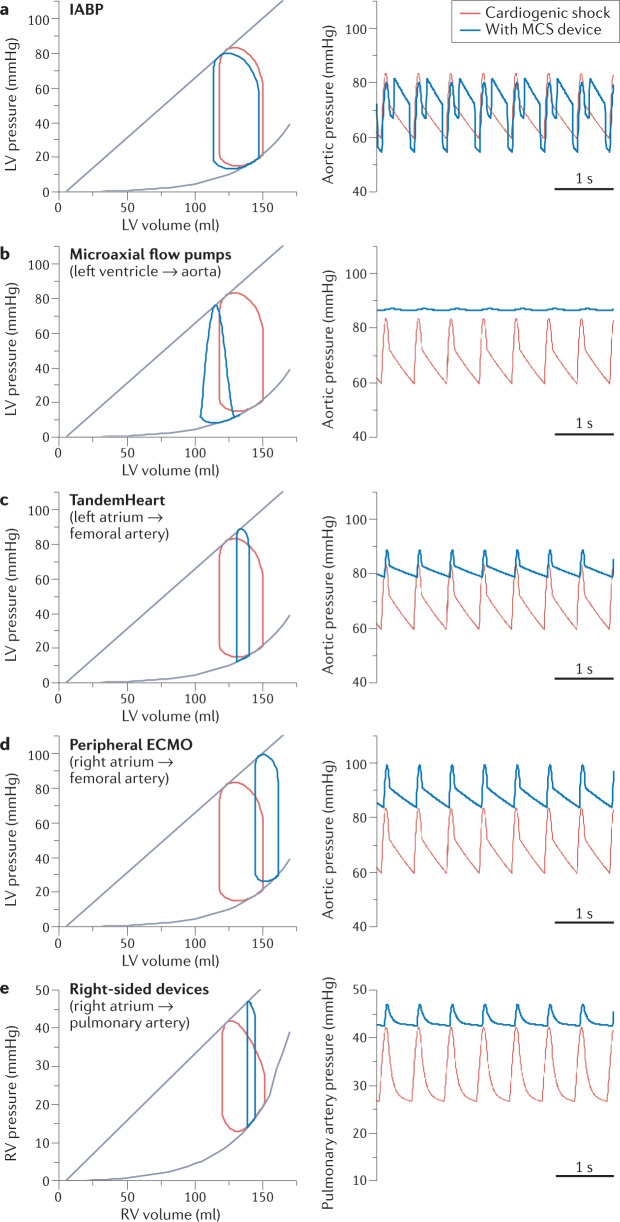
Originally intended for life-saving salvage therapy, the use of temporary mechanical circulatory support (MCS) devices has become increasingly widespread in a variety of clinical settings in the contemporary era. Their use as a short-term, prophylactic support vehicle has expanded to include procedures in the catheterization laboratory, electrophysiology suite, operating room and intensive care unit. Accordingly, MCS device design and technology continue to develop at a rapid pace. In this Review, we describe the functionality, indications, management and complications associated with temporary MCS, together with scenario-specific utilization, goal-directed development and bioengineering of future devices. We address various considerations for the use of temporary MCS devices in both prophylactic and rescue scenarios, with input from stakeholders from various cardiovascular specialties, including interventional and heart failure cardiology, electrophysiology, cardiothoracic anaesthesiology, critical care and cardiac surgery.
© 2022. Springer Nature Limited.
Conflict of interest statement
S.R.D. declares receiving research grant support from Biosense Webster and owning equity in Farapulse (acquired by Boston Scientific) and Manual Surgical Sciences. D.B. declares receiving an unrestricted educational grant from Abiomed, acting as a consultant to PVLoops and receiving consulting fees from CardioDyme. A.L. declares receiving speaker honoraria from Zoll, being on a data safety and monitoring board for Sequana, being on the advisory board of Bioventrix and being a speaker for Novartis. The other authors declare no competing interests.
Figures
References
-
- Krishna M, Zacharowski K. Principles of intra-aortic balloon pump counterpulsation. Contin. Educ. Anaesth. Crit. Care Pain. 2009;9:24–28. doi: 10.1093/bjaceaccp/mkn051. - DOI
-
- Getinge. Intra-aortic balloon counterpulsation. Getingehttps://www.getinge.com/me/products/hospital/counterpulsation/ (2022).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
