

Association Between Giving Birth During the Early Coronavirus Disease 2019 (COVID-19) Pandemic and Serious Maternal Morbidity
- PMID: 36357949
- PMCID: PMC9892237
- DOI: 10.1097/AOG.0000000000004982
Association Between Giving Birth During the Early Coronavirus Disease 2019 (COVID-19) Pandemic and Serious Maternal Morbidity
Abstract
Objective: To evaluate whether delivering during the early the coronavirus disease 2019 (COVID-19) pandemic was associated with increased risk of maternal death or serious morbidity from common obstetric complications compared with a historical control period.
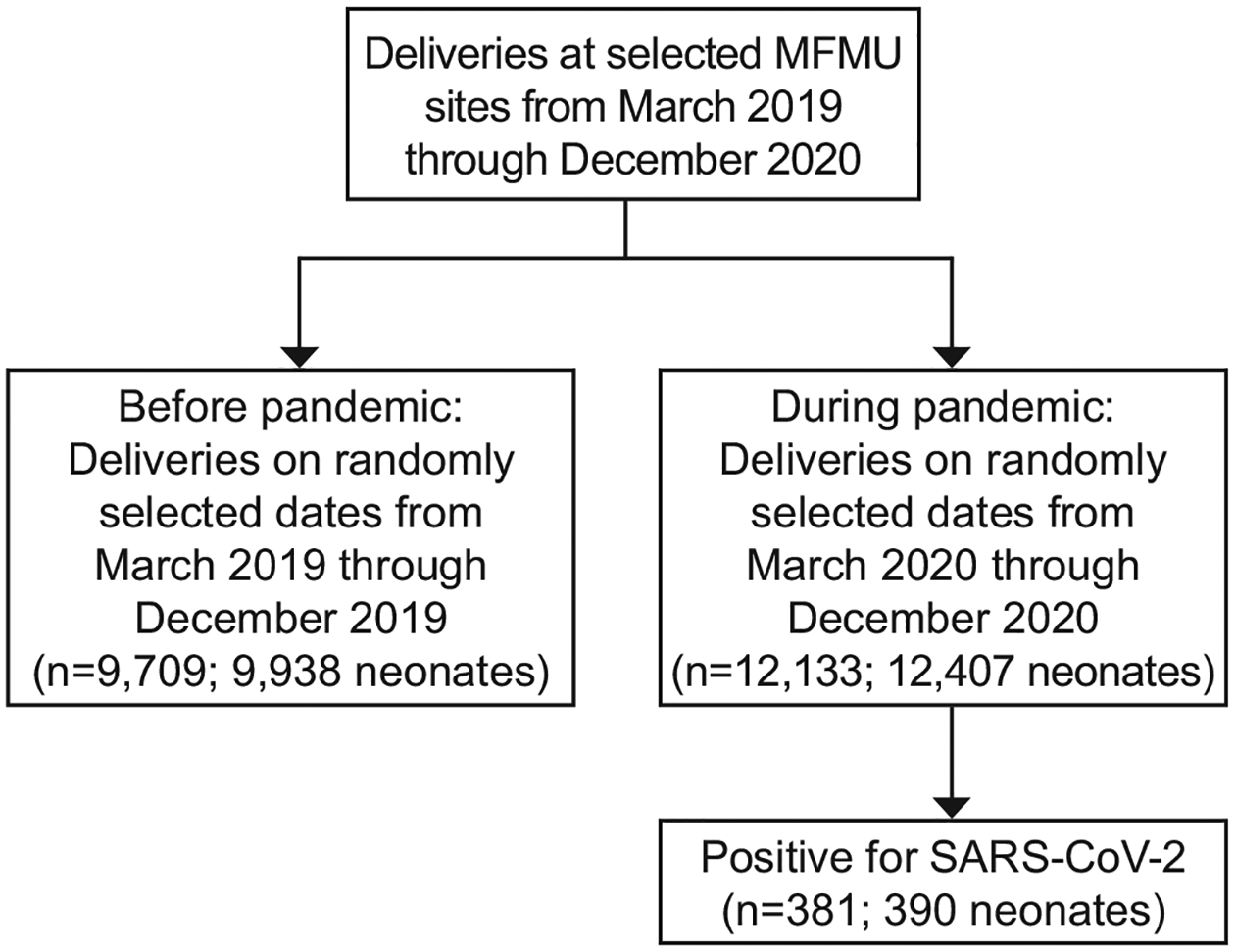
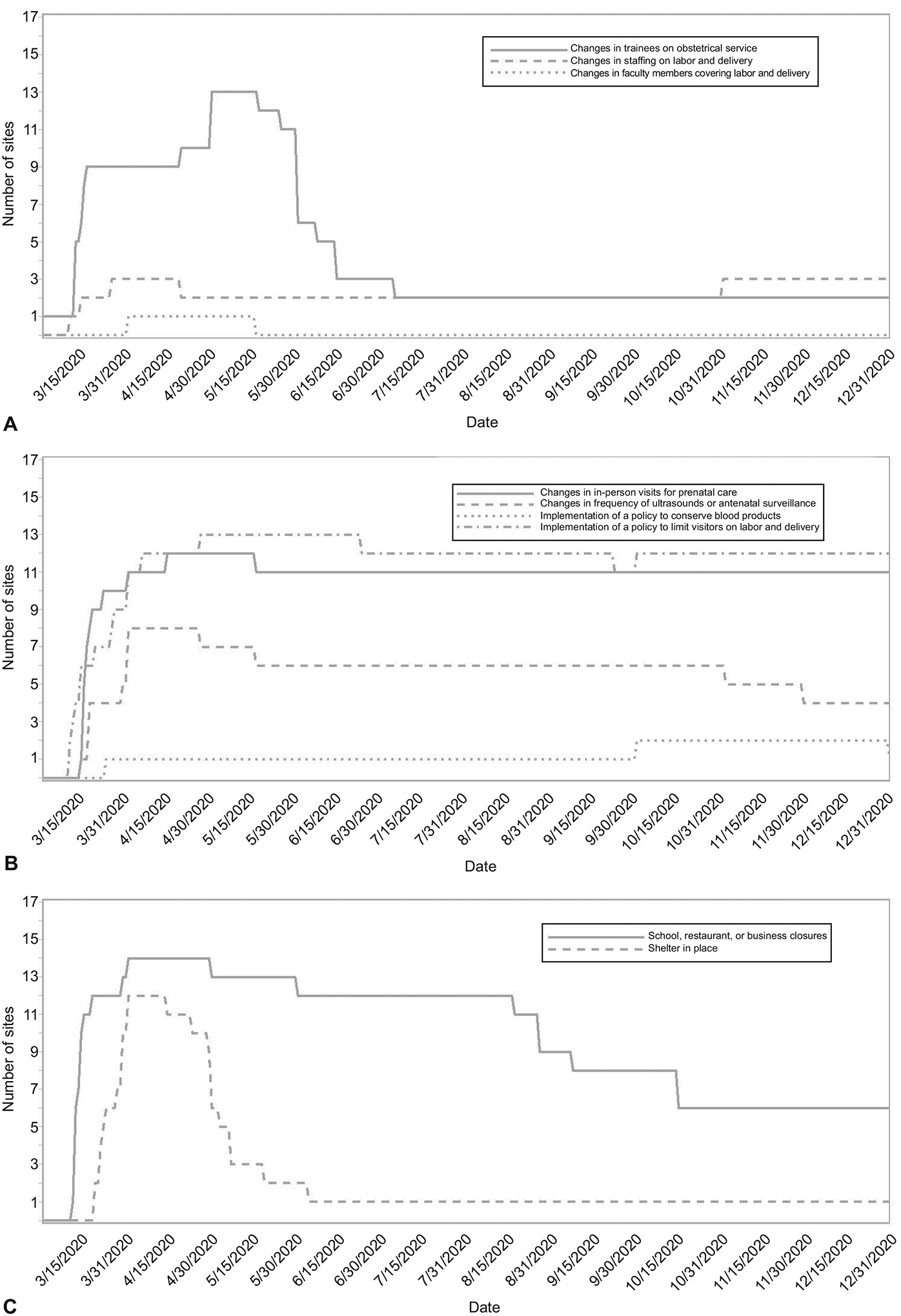
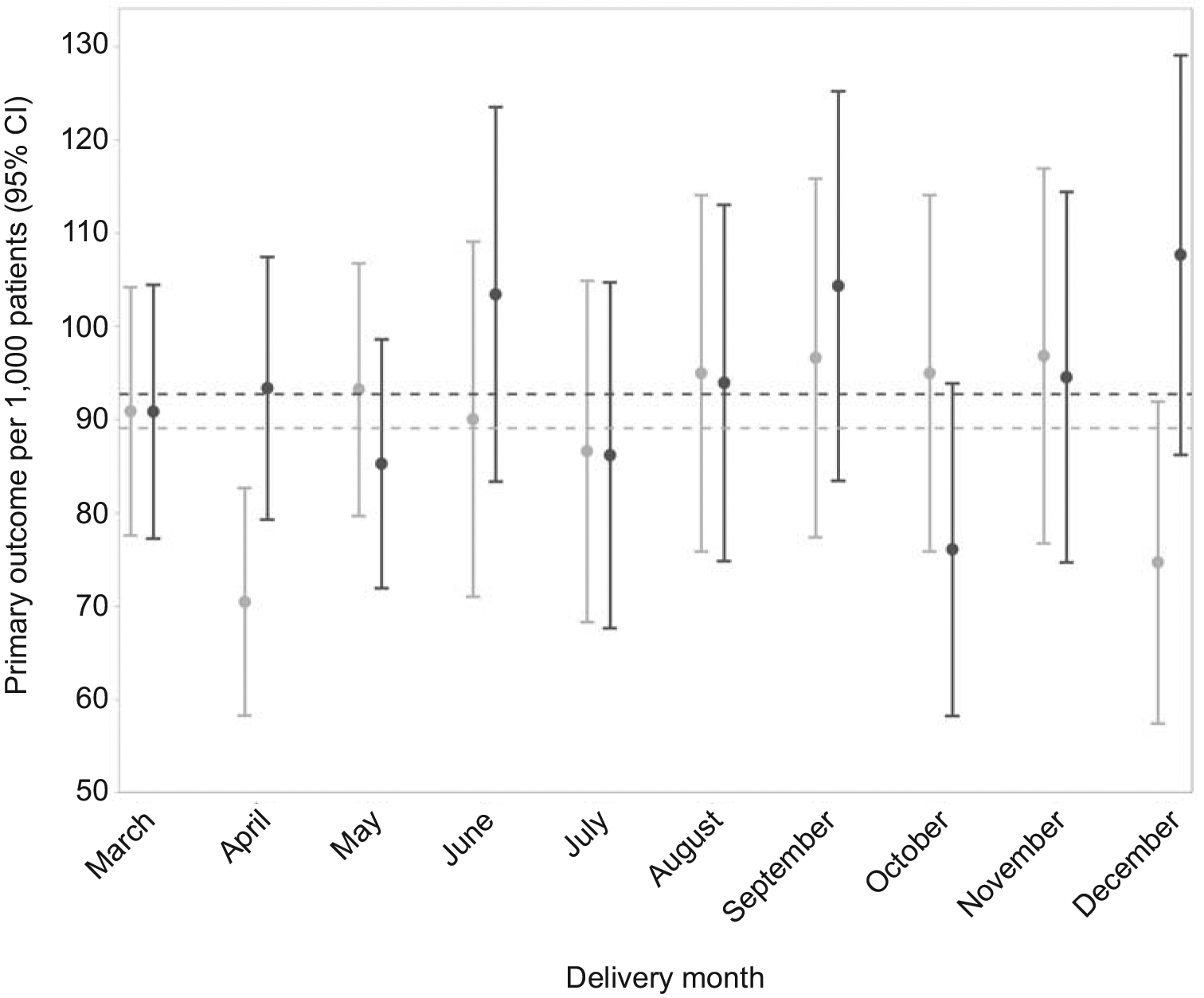
Methods: This was a multicenter retrospective cohort study with manual medical-record abstraction performed by centrally trained and certified research personnel at 17 U.S. hospitals. Individuals who gave birth on randomly selected dates in 2019 (before the pandemic) and 2020 (during the pandemic) were compared. Hospital, health care system, and community risk-mitigation strategies for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in response to the early COVID-19 pandemic are described. The primary outcome was a composite of maternal death or serious morbidity from common obstetric complications, including hypertensive disorders of pregnancy (eclampsia, end organ dysfunction, or need for acute antihypertensive therapy), postpartum hemorrhage (operative intervention or receipt of 4 or more units blood products), and infections other than SARS-CoV-2 (sepsis, pelvic abscess, prolonged intravenous antibiotics, bacteremia, deep surgical site infection). The major secondary outcome was cesarean birth.
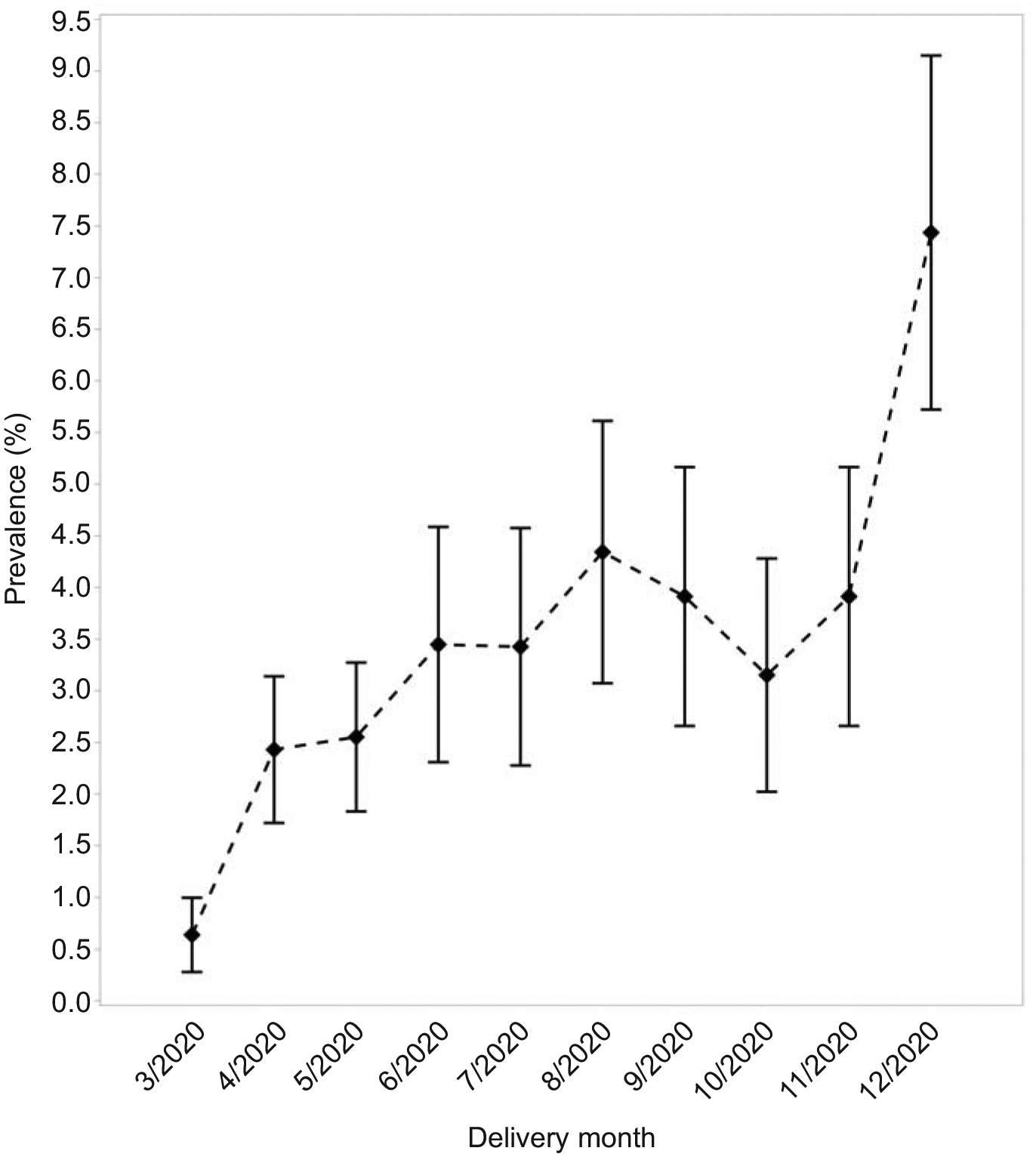
Results: Overall, 12,133 patients giving birth during and 9,709 before the pandemic were included. Hospital, health care system, and community SARS-CoV-2 mitigation strategies were employed at all sites for a portion of 2020, with a peak in modifications from March to June 2020. Of patients delivering during the pandemic, 3% had a positive SARS-CoV-2 test result during pregnancy through 42 days postpartum. Giving birth during the pandemic was not associated with a change in the frequency of the primary composite outcome (9.3% vs 8.9%, adjusted relative risk [aRR] 1.02, 95% CI 0.93-1.11) or cesarean birth (32.4% vs 31.3%, aRR 1.02, 95% CI 0.97-1.07). No maternal deaths were observed.
Conclusion: Despite substantial hospital, health care, and community modifications, giving birth during the early COVID-19 pandemic was not associated with higher rates of serious maternal morbidity from common obstetric complications.
Clinical trial registration: ClinicalTrials.gov, NCT04519502.
Copyright © 2022 by the American College of Obstetricians and Gynecologists. Published by Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
Financial Disclosure Torri D. Metz reports personal fees from Pfizer for her role as a medical consultant for a SARS-CoV-2 vaccination in pregnancy study, grants from Pfizer for role as a site PI for SARS-CoV-2 vaccination in pregnancy study, grants from Pfizer for role as a site PI for RSV vaccination in pregnancy study, and grants from Gestvision for role as a site PI for a preeclampsia study outside the submitted work. Brenna L. Hughes reports personal fees from Merck for her role on a Medical Advisory Board outside of the submitted work. Tracy A. Manuck reports money was paid to her institution from the NIH (NICHD and NIEHS) and the State of North Carolina (PFAST Network Grant). She also received Cefalo Bowes grant funding (local UNC obgyn grant funding) where she was a mentor to fellow physicians. Hyagriv N. Simhan reports that he is an LLC Co-founder of Naima Health and personal fees from UpToDate outside of the submitted work. Cynthia Gyamfi-Bannerman reports receiving payment from Medela and Hologic. Alan T.N. Tita reports grants from CDC and from Pfizer for a COVID-19 in pregnancy trial outside of the submitted work. The other authors did not report any potential conflicts of interest.
Figures
References
-
- Hoyert DL. Maternal mortality rates in the United States, 2020. NCHS Health E-Stats. 2022. DOI: 10.15620/cdc:113967. - DOI
Publication types
MeSH terms
Associated data
Grants and funding
- UG1 HD027869/HD/NICHD NIH HHS/United States
- UG1 HD040560/HD/NICHD NIH HHS/United States
- UG1 HD087230/HD/NICHD NIH HHS/United States
- UG1 HD053097/HD/NICHD NIH HHS/United States
- UG1 HD040545/HD/NICHD NIH HHS/United States
- UG1 HD040485/HD/NICHD NIH HHS/United States
- U10 HD034208/HD/NICHD NIH HHS/United States
- UG1 HD040500/HD/NICHD NIH HHS/United States
- UL1 TR001873/TR/NCATS NIH HHS/United States
- UG1 HD027915/HD/NICHD NIH HHS/United States
- UG1 HD087192/HD/NICHD NIH HHS/United States
- UG1 HD040544/HD/NICHD NIH HHS/United States
- UG1 HD034208/HD/NICHD NIH HHS/United States
- UG1 HD040512/HD/NICHD NIH HHS/United States
- U10 HD036801/HD/NICHD NIH HHS/United States
- U24 HD036801/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
