

Prompt and Appropriate Antimicrobial Therapy Improves Outcomes of NDM-Producing and KPC-Producing Klebsiella pneumoniae Bloodstream Infections in Patients Hospitalized for COVID-19: A Comparative Retrospective Case-Series
- PMID: 36358174
- PMCID: PMC9686740
- DOI: 10.3390/antibiotics11111519
Prompt and Appropriate Antimicrobial Therapy Improves Outcomes of NDM-Producing and KPC-Producing Klebsiella pneumoniae Bloodstream Infections in Patients Hospitalized for COVID-19: A Comparative Retrospective Case-Series
Abstract
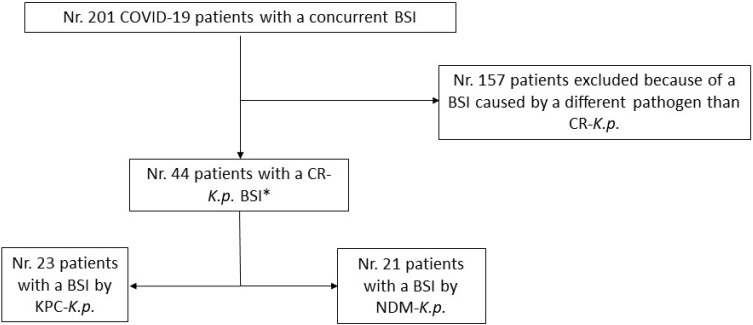
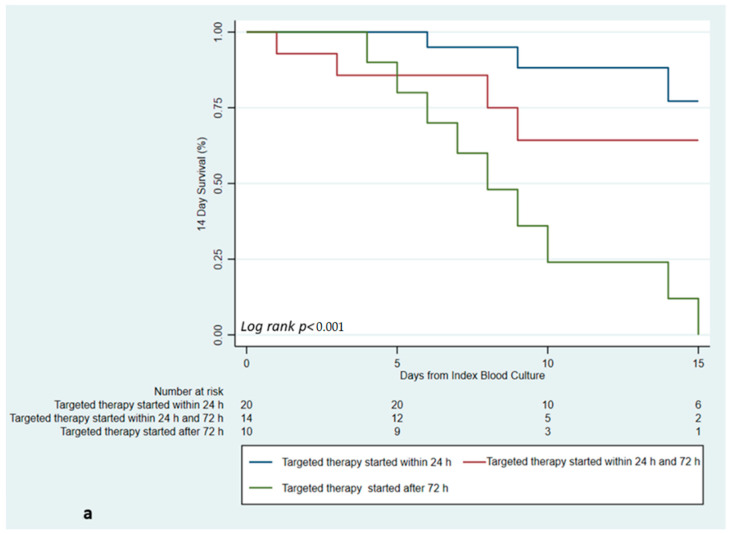
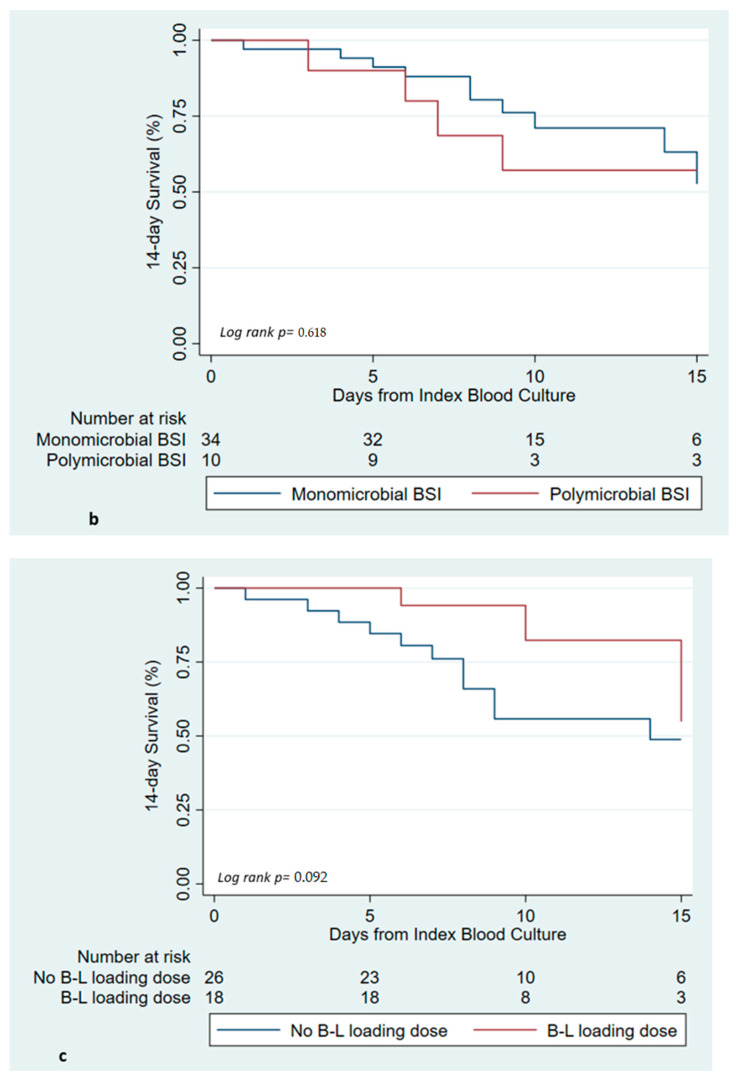
Secondary bloodstream infections (BSIs) caused by KPC- and NDM-producing Klebsiella pneumoniae (K.p.) during the course of COVID-19 infections lead to significant mortality. Herein, a comparative retrospective case series of KPC- or NDM-K.p. BSIs occurring in COVID-19 subjects treated with Ceftazidime/Avibactam (CAZ/AVI) for KPC-K.p., or CAZ/AVI+ Aztreonam (ATM) for NDM-K.p is reported. All patients hospitalized for COVID-19 in two Italian hospitals with a BSI between March and September 2021 were included. The main outcome was 14-day mortality. Overall, 44 patients were included: 23 with KPC-K.p. and 21 with NDM-K.p. BSIs. The median (q1-q3) age was 67 (57-75) years, and 32 (72%) were males. The two groups were similar in terms of baseline comorbidity, or severity of COVID-19. Notably, 14-day mortality of KPC-K.p. BSIs and NDM-K.p. BSIs (26% vs. 38%, p = 0.521) and 28-day mortality (35% vs. 48%, p = 0.541) were similar. A Cox regression model of delayed initiation of an appropriate antibiotic therapy after the onset of symptoms independently predicted mortality: initiation between 24 and 72 h (aHR = 12.03; 95% CI = 1.10-130, p = 0.041); and initiation after 72h (aHR = 36.9, 95% CI = 3.22-424, p = 0.004). Moreover, a trend towards an increased risk of mortality was observed for polymicrobial infections (aHR = 3.73, 95% CI = 0.87-15.8, p = 0.074), while a protective effect was observed for a beta-lactam loading dose at the start of treatment (aHR = 0.16, 95% CI = 0.02-1.10, p = 0.064). The high mortality of KPC and NDM-K.p. BSIs in COVID-19 patients may be reduced by an early and appropriate antibiotic therapy. Further efforts should be made to develop antimicrobial stewardship and infection control programs in COVID-19 wards.
Keywords: COVID-19; KPC-Klebsiella pneumoniae; NDM-Klebsiella pneumoniae; SARS-CoV2; bloodstream infections.
Conflict of interest statement
No author has any conflict of interest to declare related to the article.
Figures
References
-
- Ammerlaan H.S., Harbarth S., Buiting A.G., Crook D.W., Fitzpatrick F., Hanberger H., Herwaldt L.A., van Keulen P.H.J., Kluytmans J.A.J.W., Kola A., et al. Secular trends in nosocomial bloodstream infections: Antibiotic-resistant bacteria increase the total burden of infection. Clin. Infect. Dis. 2013;56:798–805. doi: 10.1093/cid/cis1006. - DOI - PubMed
-
- Bavaro D.F., Pizzutilo P., Catino A., Signorile F., Pesola F., Di Gennaro F., Cassiano S., Marech I., Lamorgese V., Angarano G., et al. Incidence of Infections and Predictors of Mortality During Checkpoint Inhibitor Immunotherapy in Patients with Advanced Lung Cancer: A Retrospective Cohort Study. Open Forum Infect. Dis. 2021;8:ofab187. doi: 10.1093/ofid/ofab187. - DOI - PMC - PubMed
-
- Ippolito M., Simone B., Filisina C., Catalanotto F.R., Catalisano G., Marino C., Misseri G., Giarratano A., Cortegiani A. Bloodstream Infections in Hospitalized Patients with COVID-19: A Systematic Review and Meta-Analysis. Microorganisms. 2021;9:2016. doi: 10.3390/microorganisms9102016. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
