

Hyperlipoproteinemia(a) and Severe Coronary Artery Lesion Types
- PMID: 36359368
- PMCID: PMC9687572
- DOI: 10.3390/biomedicines10112848
Hyperlipoproteinemia(a) and Severe Coronary Artery Lesion Types
Abstract
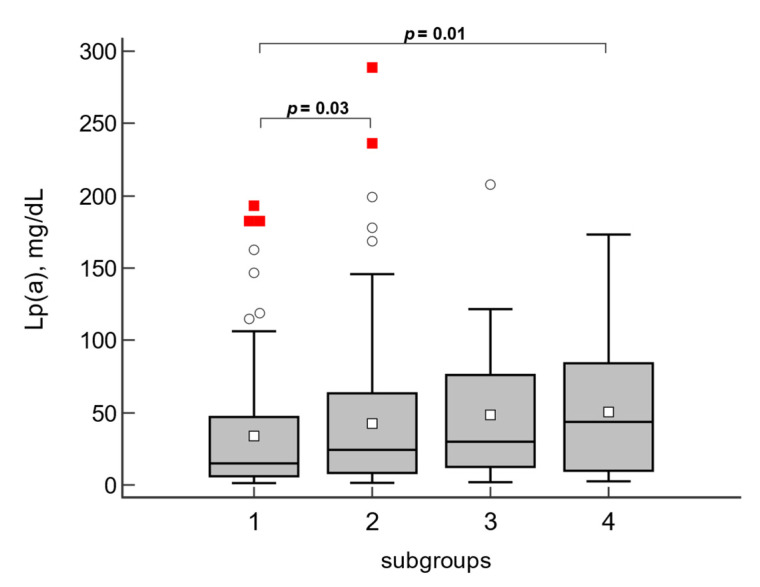
Diffuse atherosclerosis and calcification of the coronary arteries (CA) create serious difficulties for coronary artery bypass grafting (CABG). The aim of this study was to compare demographic indicators, lipids, and clinical results one year after CABG in patients with different phenotypes of coronary artery (CA) disease. In total, 390 patients hospitalized for elective CABG were included in a single-center prospective study. Demographic data, lipids (total, low-density lipoprotein and high-density lipoprotein cholesterol, and triglycerides), and lipoprotein(a) (Lp(a)) concentrations were analyzed for all patients. Major adverse cardiovascular events (MACE) included myocardial infarction, stroke, percutaneous coronary intervention, and death from cardiac causes within one year after surgery. No significant outcome differences were found between the groups with diffuse vs. segmental lesions, nor the groups with and without calcinosis for all studied parameters except for Lp(a). Median Lp(a) concentrations were higher in the group of patients with diffuse compared to segmental lesions (28 vs. 16 mg/dL, p = 0.023) and in the group with calcinosis compared to the group without it (35 vs. 19 mg/dL, p = 0.046). Lp(a) ≥ 30 mg/dL was associated with the presence of diffuse lesions (OR = 2.18 (95% CI 1.34-3.54), p = 0.002), calcinosis (2.15 (1.15-4.02), p = 0.02), and its combination (4.30 (1.81-10.19), p = 0.0009), irrespective of other risk factors. The risk of MACE within one year after CABG was higher for patients with combined diffuse and calcified lesions vs. patients with a segmental lesion without calcinosis (relative risk = 2.38 (1.13-5.01), p = 0.02). Conclusion: Diffuse atherosclerosis and coronary calcinosis are associated with elevated Lp(a) levels, independent of other risk factors. The risk of MACE in the first year after surgery is significantly higher in patients with diffuse atherosclerosis and coronary calcinosis, which should be considered when prescribing postoperative treatment for such patients.
Keywords: coronary artery calcinosis; coronary bypass grafting; diffuse atherosclerosis; lipoprotein(a).
Conflict of interest statement
The authors declare no conflict of interest.
Figures



References
-
- Willeit P., Ridker P.M., Nestel P.J., Simes J., Tonkin A.M., Pedersen T.R., Schwartz G.G., Olsson A.G., Colhoun H.M., Kronenberg F., et al. Baseline and on-statin treatment lipoprotein(a) levels for prediction of cardiovascular events: Individual patient-data meta-analysis of statin outcome trials. Lancet. 2018;392:1311–1320. doi: 10.1016/S0140-6736(18)31652-0. - DOI - PubMed
-
- Kronenberg F., Mora S., Stroes E.S.G., Ference B.A., Arsenault B.J., Berglund L., Dweck M.R., Koschinsky M., Lambert G., Mach F., et al. Lipoprotein(a) in atherosclerotic cardiovascular disease and aortic stenosis: A European Atherosclerosis Society consensus statement. Eur. Heart J. 2022;43:3925–3946. doi: 10.1093/eurheartj/ehac361. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
