

Review
doi: 10.3390/diagnostics12112594.
PSMA PET-CT in the Diagnosis and Staging of Prostate Cancer
Affiliations
- PMID: 36359439
- PMCID: PMC9689635
- DOI: 10.3390/diagnostics12112594
Item in Clipboard
Review
PSMA PET-CT in the Diagnosis and Staging of Prostate Cancer
Diagnostics (Basel).
.
Abstract
Prostate cancer is the most common cancer and the second leading cause of cancer death in men. The imaging assessment and treatment of prostate cancer has vastly improved over the past decade. The introduction of PSMA PET-CT has improved the detection of loco-regional and metastatic disease. PSMA PET-CT also has a role in the primary diagnosis and staging, in detecting biochemical recurrence after curative treatment and in metastasis-directed therapy. In this paper we review the role of PSMA PET-CT in prostate cancer.
Keywords: PSMA PET; imaging; prostate cancer.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
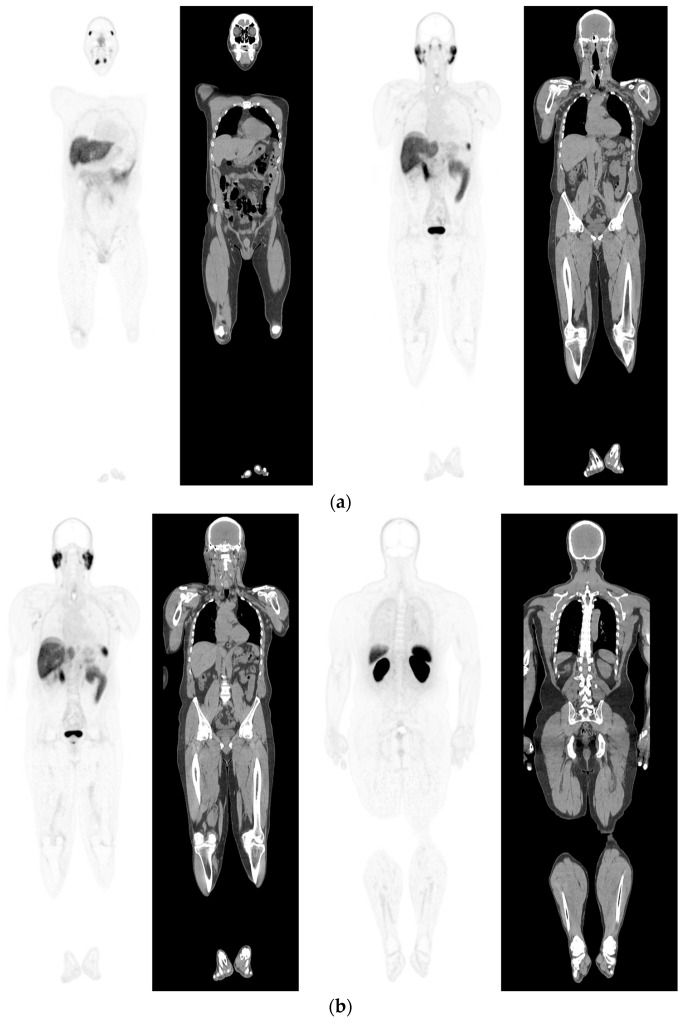
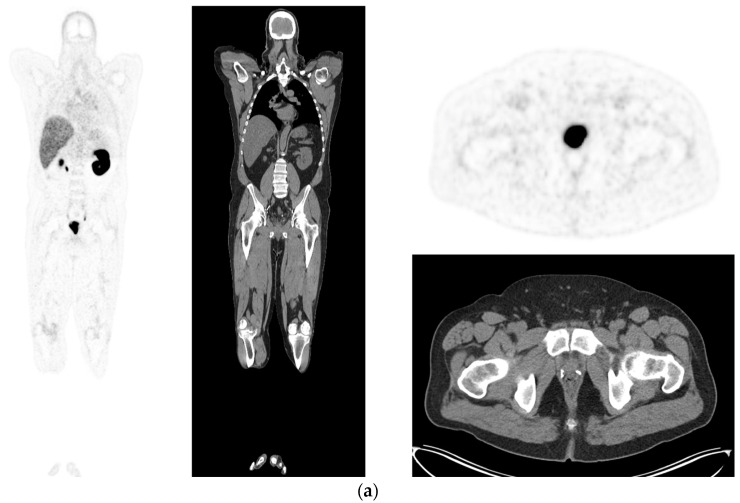
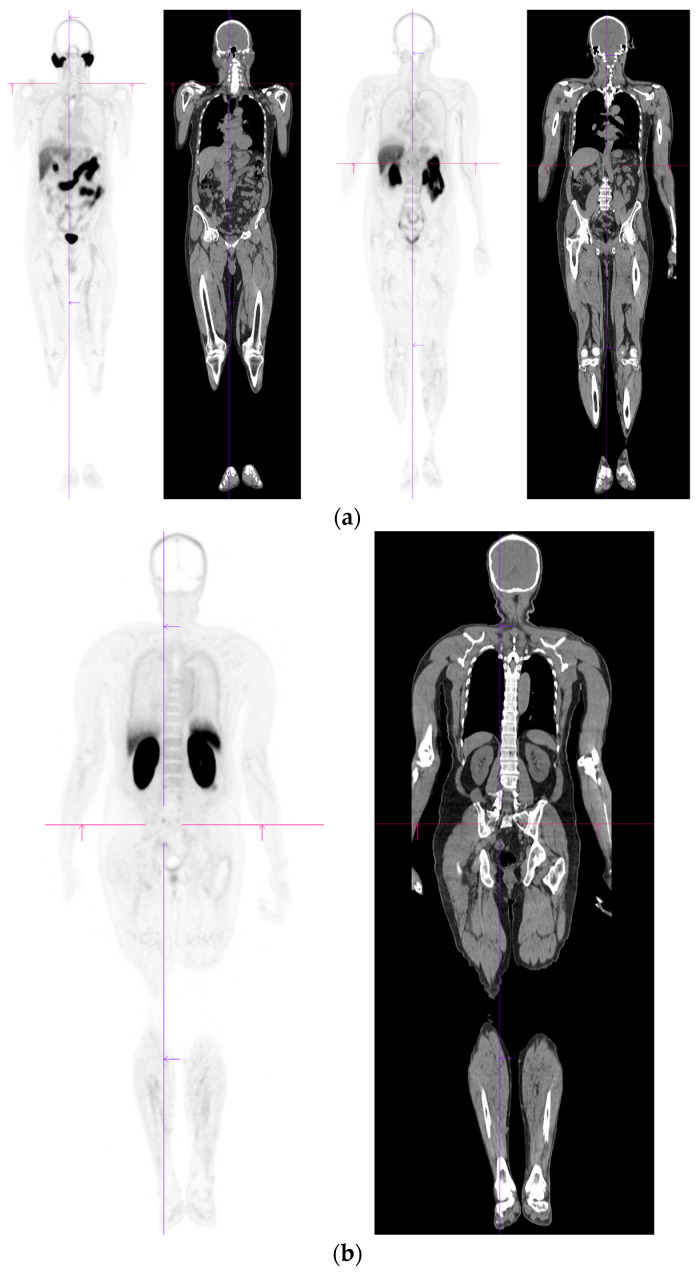
PSMA PET-CT scan showing normal distribution of PSMA-11. 60 yr old M—Gleason 6 prostate cancer on active surveillance for past 2 years; PSA 7.2; MR imaging—low grade changes PIRADS 2. PSMA PET-CT: 68Ga-PSMA - 204 MBq; uptake 52 min; BMI = 29.7; Wt 90 Kg; coronal PET and corresponding CT slices (soft tissue windows) from left to right. (a)—physiological uptake in lacrimal, submandibular salivary glands, parotid glands, retropharyngeal soft tissue, liver, bowel, part of spleen and pooling of tracer in bladder; mild reactive tracer uptake in groin and axillary nodes. (b)—physiological uptake in head and neck; reactive uptake axillary nodes; focal uptake in apex of prostate gland anterior below the bladder SUV = 9.1; marked uptake/excretion of tracer in both kidneys.
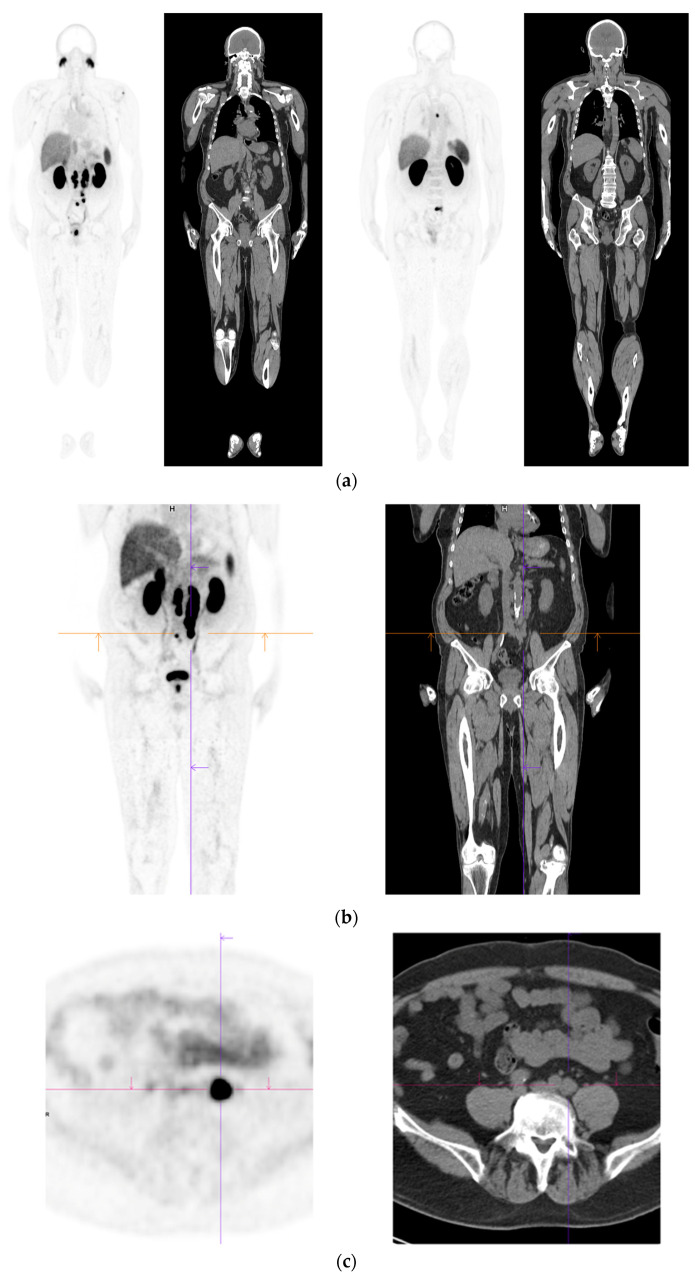
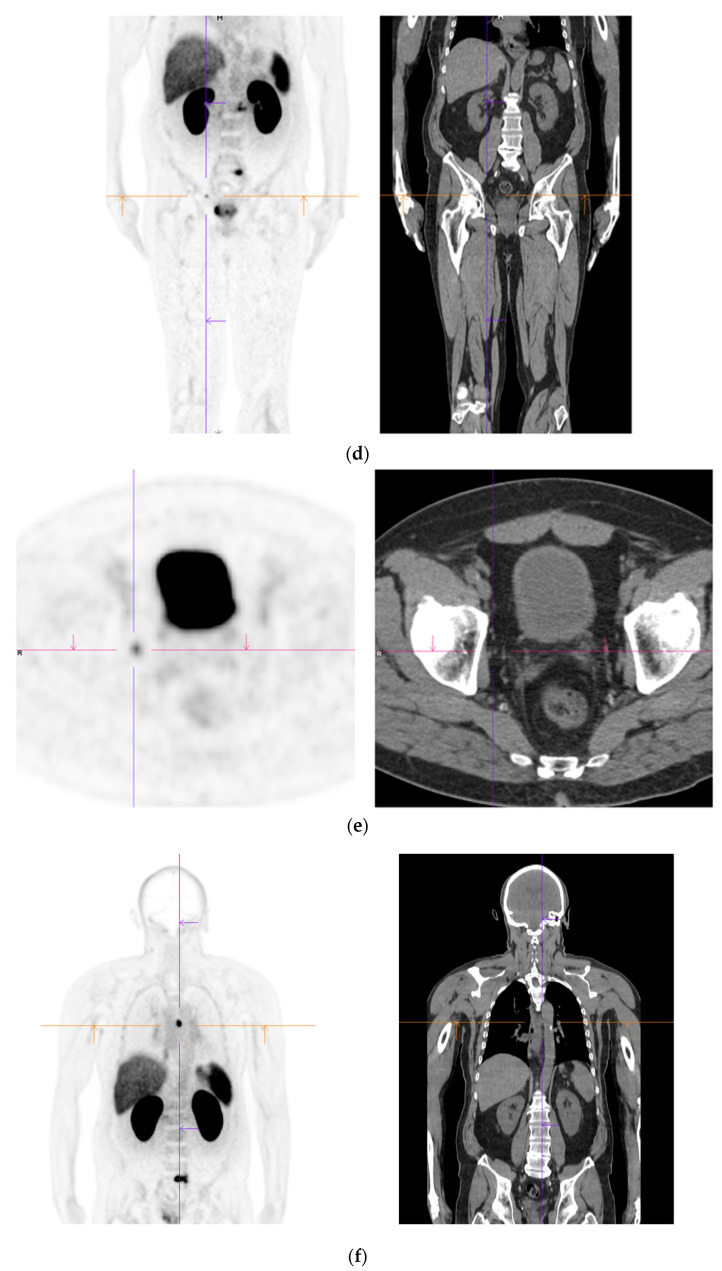
Primary staging. 70 yr old M; PSA 42; Gleason 4 + 5 = 9; MR scan—PIRADS 6 at right apex; PIRADS 4 at left midzone. PSMA PET-CT: 68Ga-PSMA - 216 MBq; uptake 48 min; BMI = 30.5; Wt 83 Kg. (a): Coronal images—focal uptake midline apex anterior SUV = 26.1 with smaller focus SUV-5.4 right midzone; bulky disease in abdominal nodes; metastasis left humerus; left para-aortic node in thorax; bony metastasis left side of S1. (b,c): enlarged coronal and transaxial images of left common iliac/para-aortic nodal disease and uptake in apex of gland; transaxial images—node measures 14 mm SUV = 40.1; X-hairs show location. (d,e): enlarged coronal and transaxial images of right pelvic nodal that measures 1.4 mm SUV = 5.1; uptake in right midzone and apex as well as disease in left midzone of gland; X-hairs show location. (f,g): enlarged coronal images of para-aortic/para-oesophageal nodal disease in mediastinum; node measures 5.5 mm, SUV = 17.2; X-hairs show location.
Primary staging. 70 yr old M; PSA 42; Gleason 4 + 5 = 9; MR scan—PIRADS 6 at right apex; PIRADS 4 at left midzone. PSMA PET-CT: 68Ga-PSMA - 216 MBq; uptake 48 min; BMI = 30.5; Wt 83 Kg. (a): Coronal images—focal uptake midline apex anterior SUV = 26.1 with smaller focus SUV-5.4 right midzone; bulky disease in abdominal nodes; metastasis left humerus; left para-aortic node in thorax; bony metastasis left side of S1. (b,c): enlarged coronal and transaxial images of left common iliac/para-aortic nodal disease and uptake in apex of gland; transaxial images—node measures 14 mm SUV = 40.1; X-hairs show location. (d,e): enlarged coronal and transaxial images of right pelvic nodal that measures 1.4 mm SUV = 5.1; uptake in right midzone and apex as well as disease in left midzone of gland; X-hairs show location. (f,g): enlarged coronal images of para-aortic/para-oesophageal nodal disease in mediastinum; node measures 5.5 mm, SUV = 17.2; X-hairs show location.
Primary staging. 70 yr old M; PSA 42; Gleason 4 + 5 = 9; MR scan—PIRADS 6 at right apex; PIRADS 4 at left midzone. PSMA PET-CT: 68Ga-PSMA - 216 MBq; uptake 48 min; BMI = 30.5; Wt 83 Kg. (a): Coronal images—focal uptake midline apex anterior SUV = 26.1 with smaller focus SUV-5.4 right midzone; bulky disease in abdominal nodes; metastasis left humerus; left para-aortic node in thorax; bony metastasis left side of S1. (b,c): enlarged coronal and transaxial images of left common iliac/para-aortic nodal disease and uptake in apex of gland; transaxial images—node measures 14 mm SUV = 40.1; X-hairs show location. (d,e): enlarged coronal and transaxial images of right pelvic nodal that measures 1.4 mm SUV = 5.1; uptake in right midzone and apex as well as disease in left midzone of gland; X-hairs show location. (f,g): enlarged coronal images of para-aortic/para-oesophageal nodal disease in mediastinum; node measures 5.5 mm, SUV = 17.2; X-hairs show location.
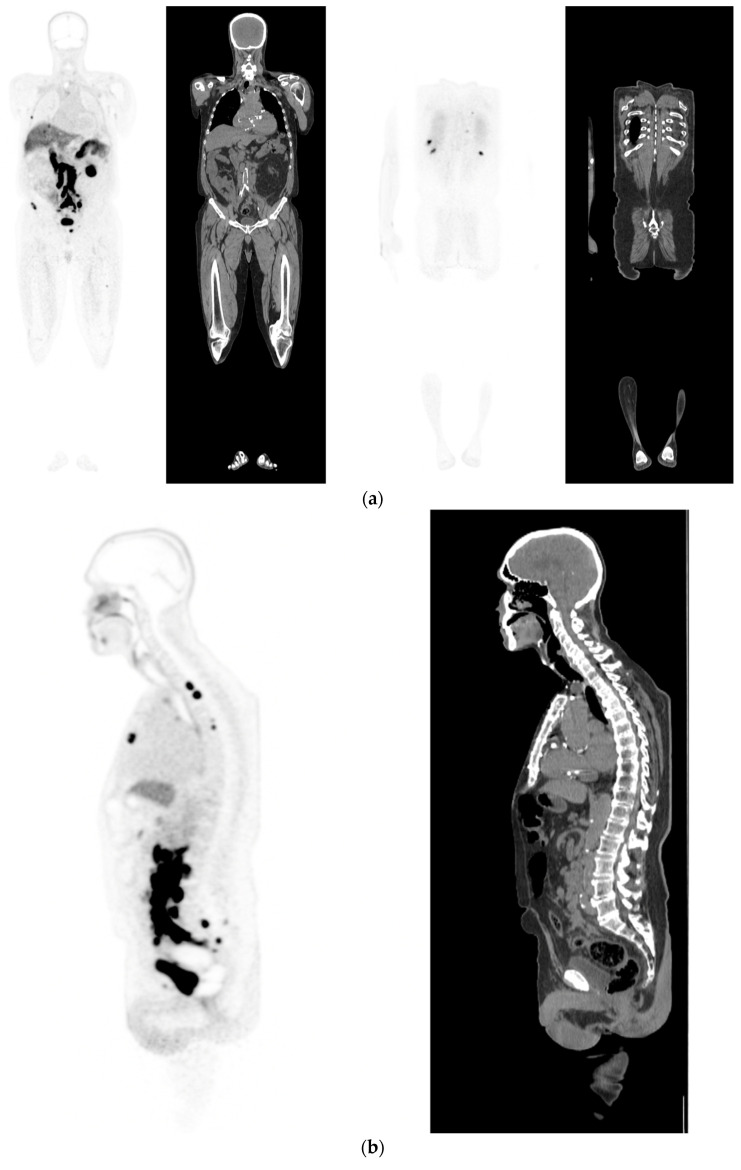
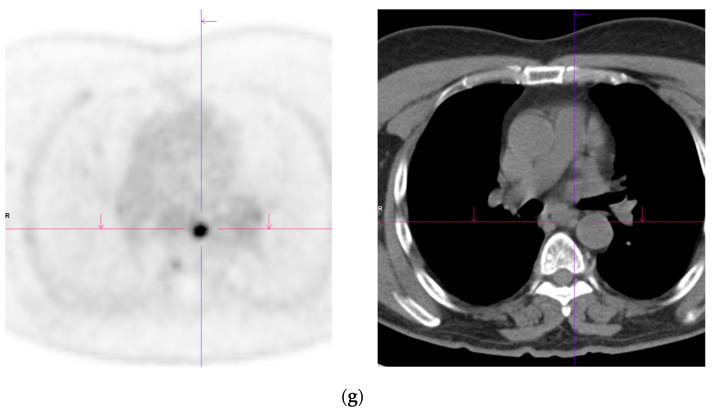
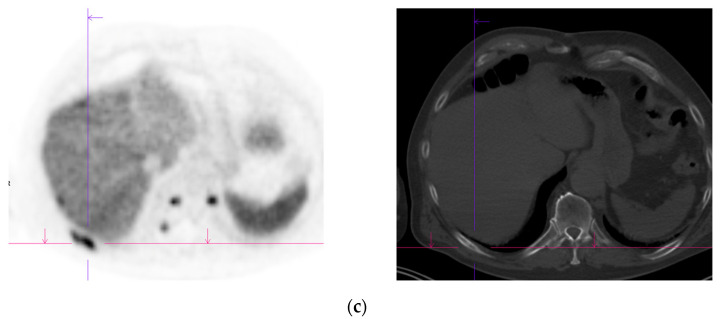
Recurrent disease. 74 yr old M; radical prostatectomy 8 yrs prior; extensive para-aortic and upper pelvic lymph node involvement on CT; severe back pain; PSA 60. PSMA PET-CT: 68Ga-PSMA-216 MBq; uptake 48 min; BMI = 31.9; Wt 89 kg. (a,b): Coronal and sagittal images show bulky nodal disease with markedly increased uptake (SUV = 68.2) in abdomen and pelvis, hepatic metastases, multiple bony metastases in pelvis, lower limbs, sternum, ribs and vertebral column. (c): enlarged transaxial images of lower thorax/upper abdomen show tracer avid foci in segments 7 (SUV = 8.8), 4 (SUV = 8.7) of liver; X-hairs on lesion in right 10th rib, SUV = 14.6; CT on bone windows shows small region of sclerosis vs. extensive uptake on PET.
Recurrent disease. 74 yr old M; radical prostatectomy 8 yrs prior; extensive para-aortic and upper pelvic lymph node involvement on CT; severe back pain; PSA 60. PSMA PET-CT: 68Ga-PSMA-216 MBq; uptake 48 min; BMI = 31.9; Wt 89 kg. (a,b): Coronal and sagittal images show bulky nodal disease with markedly increased uptake (SUV = 68.2) in abdomen and pelvis, hepatic metastases, multiple bony metastases in pelvis, lower limbs, sternum, ribs and vertebral column. (c): enlarged transaxial images of lower thorax/upper abdomen show tracer avid foci in segments 7 (SUV = 8.8), 4 (SUV = 8.7) of liver; X-hairs on lesion in right 10th rib, SUV = 14.6; CT on bone windows shows small region of sclerosis vs. extensive uptake on PET.
Biochemical recurrence—serial scans. 58 yr old M—radical prostatectomy and node disSection 10 yrs prior; scans done in July 2020 when PSA 0.24 and Sep 2021 when PSA 0.38. (a): PSMA PET-CT: July 2020-68Ga-PSMA-226 MBq; uptake 49 min; BMI = 35.1; Wt 105 kg; coronal images and transaxial images at level of prostate bed show tracer excretion; rest of study clear. (b): PSMA PET-CT: Sep 2021-68Ga-PSMA-238 MBq; uptake 50 min; BMI = 35.2; Wt 107 kg; coronal images and transaxial images at level of prostate bed show tracer excretion but with a new small focus of uptake SUV= 6.0 in left side of prostate bed; rest of study clear.
Biochemical recurrence—serial scans. 58 yr old M—radical prostatectomy and node disSection 10 yrs prior; scans done in July 2020 when PSA 0.24 and Sep 2021 when PSA 0.38. (a): PSMA PET-CT: July 2020-68Ga-PSMA-226 MBq; uptake 49 min; BMI = 35.1; Wt 105 kg; coronal images and transaxial images at level of prostate bed show tracer excretion; rest of study clear. (b): PSMA PET-CT: Sep 2021-68Ga-PSMA-238 MBq; uptake 50 min; BMI = 35.2; Wt 107 kg; coronal images and transaxial images at level of prostate bed show tracer excretion but with a new small focus of uptake SUV= 6.0 in left side of prostate bed; rest of study clear.
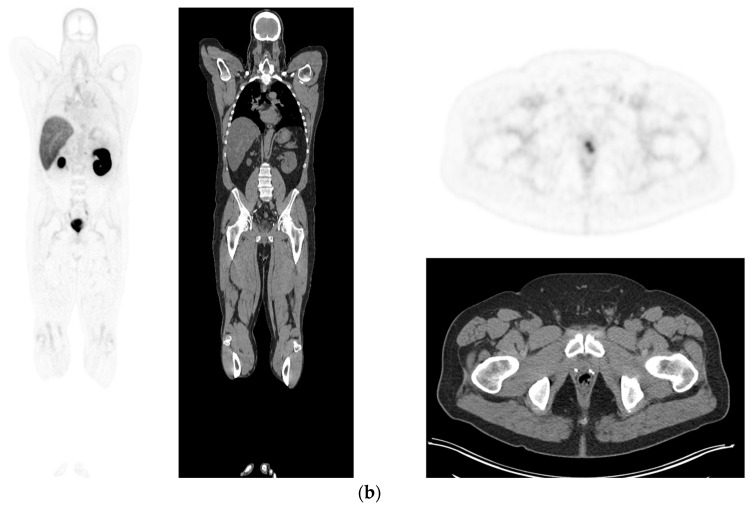
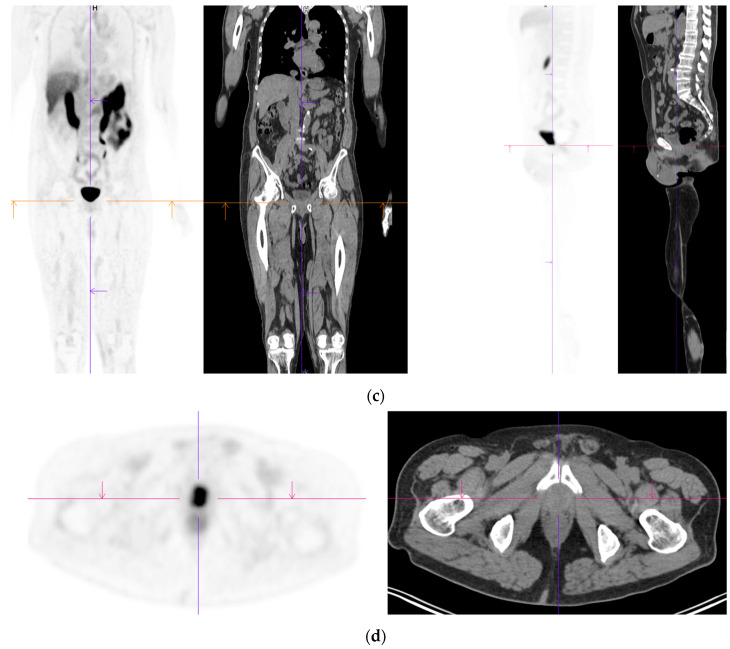
Biochemical recurrence—negative scan; normal distribution of tracer. 75 yr old M—radical prostatectomy 7 yrs prior; PSA 0.42. PSMA PET-CT: 68Ga-PSMA - 219 MBq; uptake 48 min; BMI = 22.6; Wt 63 kg. (a,b): coronal images show physiological uptake in parotid glands, bowel and kidneys and tracer pooling in bladder; X-hairs show uptake in cervical (SUV = 2.3) and sacral (SUV = 2.5) nerve roots and sympathetic ganglia in upper abdomen SUV = 4.6. (c,d): enlarged coronal, sagittal and transaxial images of prostate bed; X-hairs identify locations; no abnormal tracer uptake but pooling of trace in bladder problematic; Note—scale in sagittal images on (c) has been deliberately altered to ensure there are no adjacent focal regions of uptake to suggest local tumor recurrence.
Biochemical recurrence—negative scan; normal distribution of tracer. 75 yr old M—radical prostatectomy 7 yrs prior; PSA 0.42. PSMA PET-CT: 68Ga-PSMA - 219 MBq; uptake 48 min; BMI = 22.6; Wt 63 kg. (a,b): coronal images show physiological uptake in parotid glands, bowel and kidneys and tracer pooling in bladder; X-hairs show uptake in cervical (SUV = 2.3) and sacral (SUV = 2.5) nerve roots and sympathetic ganglia in upper abdomen SUV = 4.6. (c,d): enlarged coronal, sagittal and transaxial images of prostate bed; X-hairs identify locations; no abnormal tracer uptake but pooling of trace in bladder problematic; Note—scale in sagittal images on (c) has been deliberately altered to ensure there are no adjacent focal regions of uptake to suggest local tumor recurrence.
References
-
- Royal Australian College of General Practitioners. National Preventive and Community Medicine Committee . Guidelines for Preventive Activities in General Practice. 9th ed. RACGP; East Melbourne, Australia: 2016. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
