

A Novel Ultrasonographic Anthropometric-Independent Measurement of Median Nerve Swelling in Carpal Tunnel Syndrome: The "Nerve/Tendon Ratio" (NTR)
- PMID: 36359465
- PMCID: PMC9689936
- DOI: 10.3390/diagnostics12112621
A Novel Ultrasonographic Anthropometric-Independent Measurement of Median Nerve Swelling in Carpal Tunnel Syndrome: The "Nerve/Tendon Ratio" (NTR)
Abstract
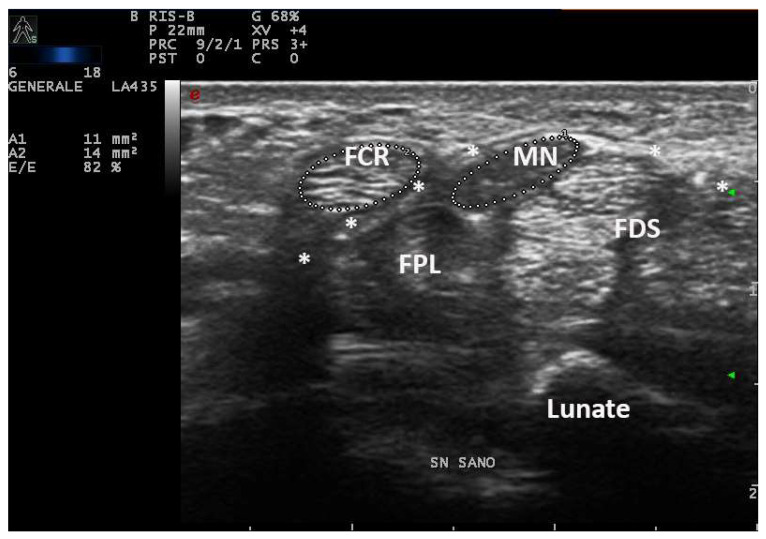
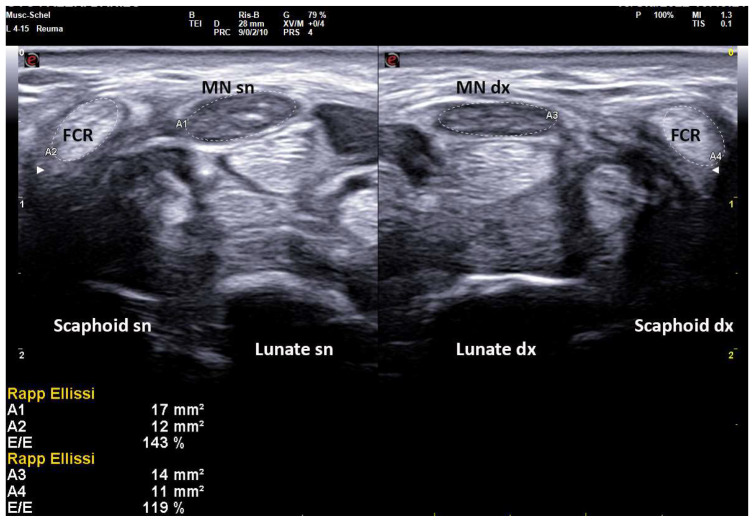
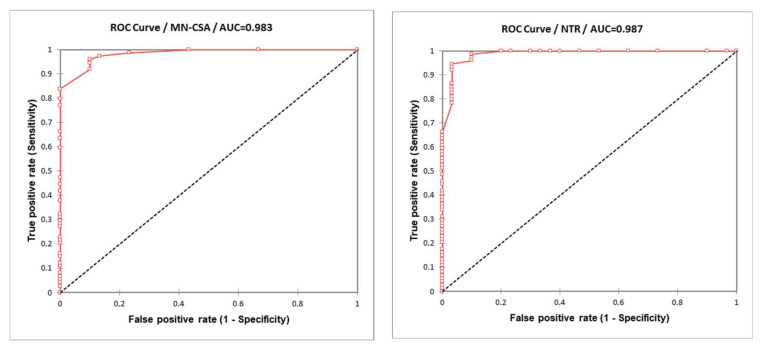
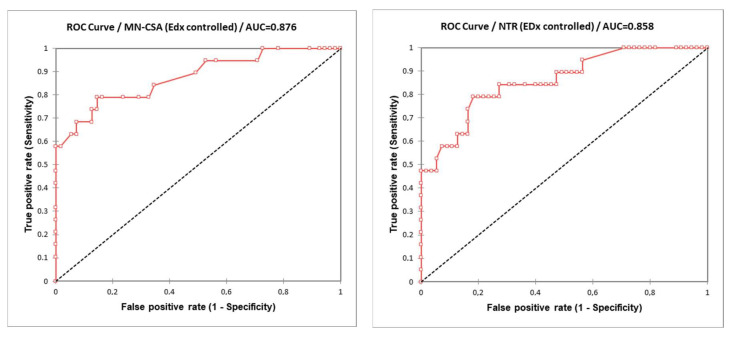
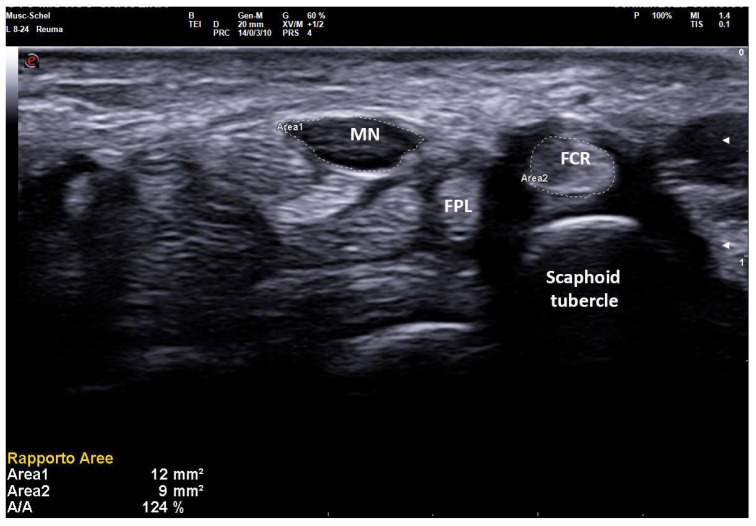
Background: There is little consensus on ultrasound (US) normative values of cross-sectional area of median nerve (MN-CSA) in carpal tunnel syndrome (CTS) because of its dependency on anthropometric parameters. We aim to propose a novel anthropometric-independent US parameter: MN-CSA/flexor radialis carpi CSA (FCR-CSA) ratio (“Nerve Tendon Ratio”, NTR), in the diagnosis of clinically and electrodiagnostic (EDS)-defined CTS. Methods: 74 wrists of 49 patients with clinically defined CTS underwent EDS (scored by the 1−5 Padua Scale of electrophysiological severity, PS) and US of carpal tunnel with measurement of MN-CSA (at the carpal tunnel inlet), FCR-CSA (over scaphoid tubercle) and its ratio (NTR, expressed as a percentage). US normality values and intra-operator agreement were assessed in 33 healthy volunteers. Results: In controls, the mean MN-CSA was 5.81 mm2, NTR 64.2%. In 74 clinical CTS, the mean MN-CSA was 12.1 mm2, NTR 117%. In severe CTS (PS > 3), the mean MN-CSA was 15.9 mm2, NTR 148%. In CTS, both MN-CSA and NTR correlated with sensitive conduction velocity (SCV) (p < 0.001), distal motor latency (DML) (p < 0.001) and PS (p < 0.001), with a slight superiority of NTR vs. MN-CSA when controlled for height, wrist circumference and weight. In CTS filtered for anthropometric extremes, only NTR maintained a correlation with SCV (p = 0.023), DML (p = 0.016) and PS (p = 0.009). Diagnostic cut-offs were obtained with a binomial regression analysis. In those patients with a clinical diagnosis of CTS, the cut-off of MN-CSA (AUROC: 0.983) was 8 mm2 (9 mm2 with highest positive predictive value, PPV), while for NTR (AUROC: 0.987), the cut-off was 83% (100% with highest PPV). In patients with EDS findings of severe CTS (PS > 3), the MN-CSA (AUROC: 0.876) cut-off was 12.3 mm2 (15.3 mm2 with highest PPV), while for NTR (AUROC: 0.858) it was 116.2% (146.0% with highest PPV). Conclusions: NTR can be simply and quickly calculated, and it can be used in anthropometric extremes.
Keywords: carpal tunnel syndrome; electrodiagnostics; median nerve; neuropathy; ultrasound.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Pelosi L., Arányi Z., Beekman R., Bland J., Coraci D., Hobson-Webb L.D., Padua L., Podnar S., Simon N., van Alfen N., et al. Expert consensus on the combined investigation of carpal tunnel syndrome with electrodiagnostic tests and neuromuscular ultrasound. Clin. Neurophysiol. 2022;135:107–116. doi: 10.1016/j.clinph.2021.12.012. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Medical
Research Materials
