

Carotid Plaque Features and Inflammatory Biomarkers as Predictors of Restenosis and Mortality Following Carotid Endarterectomy
- PMID: 36360814
- PMCID: PMC9654888
- DOI: 10.3390/ijerph192113934
Carotid Plaque Features and Inflammatory Biomarkers as Predictors of Restenosis and Mortality Following Carotid Endarterectomy
Abstract
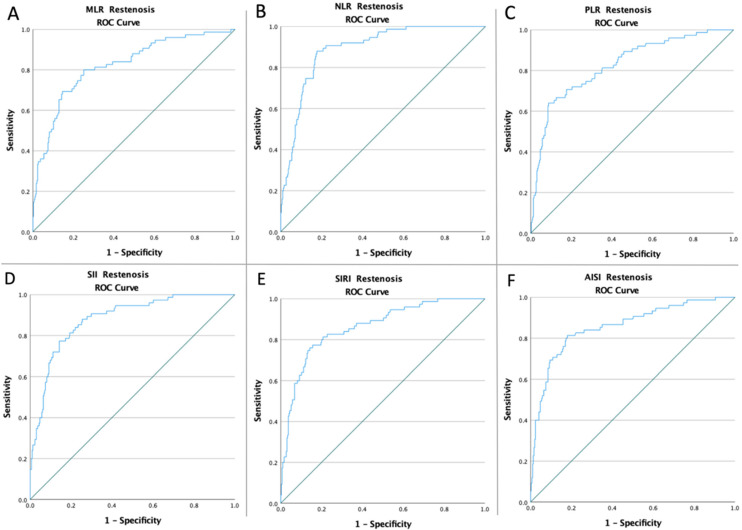
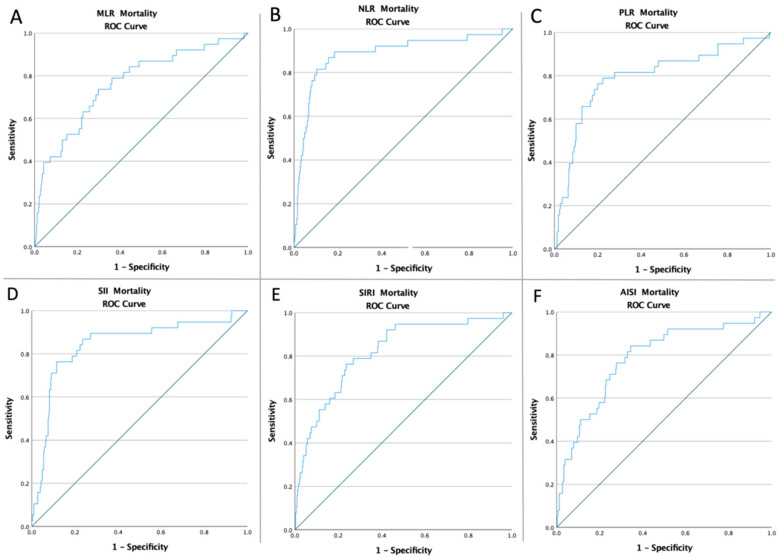
Background: Carotid endarterectomy (CEA) is the first-line surgical intervention for cases of severe carotid stenoses. Unfortunately, the restenosis rate is high after CEA. This study aims to demonstrate the predictive role of carotid plaque features and inflammatory biomarkers (monocyte-to-lymphocyte ratio (MLR), neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), systemic inflammatory index (SII), Systemic Inflammation Response Index (SIRI), and Aggregate Index of Systemic Inflammation (AISI)) in carotid restenosis and mortality at 12 months following CEA.
Methods: The present study was designed as an observational, analytical, retrospective cohort study and included all patients over 18 years of age with a minimum of 70% carotid stenosis and surgical indications for CEA admitted to the Vascular Surgery Clinic, Emergency County Hospital of Targu Mures, Romania between 2018 and 2021.
Results: According to our results, the high pre-operative values of inflammatory biomarkers-MLR (OR: 10.37 and OR: 6.11; p < 0.001), NLR (OR: 34.22 and OR: 37.62; p < 0.001), PLR (OR: 12.02 and OR: 16.06; p < 0.001), SII (OR: 18.11 and OR: 31.70; p < 0.001), SIRI (OR: 16.64 and OR: 9.89; p < 0.001), and AISI (OR: 16.80 and OR: 8.24; p < 0.001)-are strong independent factors predicting the risk of 12-month restenosis and mortality following CEA. Moreover, unstable plaque (OR: 2.83, p < 0.001 and OR: 2.40, p = 0.04) and MI (OR: 3.16, p < 0.001 and OR: 2.83, p = 0.005) were independent predictors of all outcomes. Furthermore, AH (OR: 2.30; p = 0.006), AF (OR: 1.74; p = 0.02), tobacco (OR: 2.25; p < 0.001), obesity (OR: 1.90; p = 0.02), and thrombotic plaques (OR: 2.77; p < 0.001) were all independent predictors of restenosis, but not for mortality in all patients. In contrast, antiplatelet (OR: 0.46; p = 0.004), statin (OR: 0.59; p = 0.04), and ezetimibe (OR:0.45; p = 0.03) therapy were protective factors against restenosis, but not for mortality.
Conclusions: Our data revealed that higher preoperative inflammatory biomarker values highly predict 12-month restenosis and mortality following CEA. Furthermore, age above 70, unstable plaque, cardiovascular disease, and dyslipidemia were risk factors for all outcomes. Additionally, AH, AF, smoking, and obesity were all independent predictors of restenosis but not of mortality in all patients. Antiplatelet and statin medication, on the other hand, were protective against restenosis but not against mortality.
Keywords: AISI; MLR; NLR; PLR; SII; SIRI; biomarkers; carotid plaque; carotid restenosis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Tsao C.W., Aday A.W., Almarzooq Z.I., Alonso A., Beaton A.Z., Bittencourt M.S., Boehme A.K., Buxton A.E., Carson A.P., Commodore-Mensah Y., et al. Heart Disease and Stroke Statistics—2022 Update: A Report From the American Heart Association. Circulation. 2022;145:e153–e639. doi: 10.1161/CIR.0000000000001052. - DOI - PubMed
-
- Feigin V.L., Stark B.A., Johnson C.O., Roth G.A., Bisignano C., Abady G.G., Abbasifard M., Abbasi-Kangevari M., Abd-Allah F., Abedi V., et al. Global, Regional, and National Burden of Stroke and Its Risk Factors, 1990–2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021;20:795–820. doi: 10.1016/S1474-4422(21)00252-0. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
