

Postconditioning by Delayed Administration of Ciclosporin A: Implication for Donation after Circulatory Death (DCD)
- PMID: 36361649
- PMCID: PMC9657531
- DOI: 10.3390/ijms232112858
Postconditioning by Delayed Administration of Ciclosporin A: Implication for Donation after Circulatory Death (DCD)
Abstract
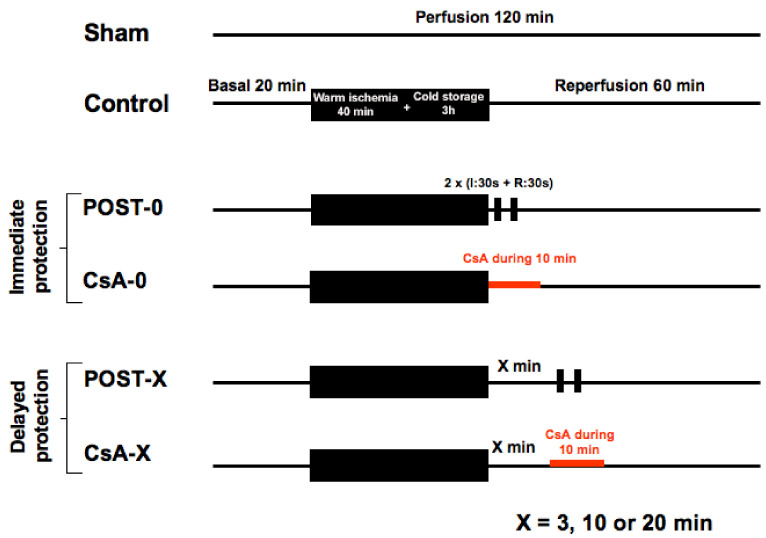
Heart transplantation is facing a shortage of grafts. Donation after Circulatory Death (DCD) would constitute a new potential of available organs. In the present work, we aimed to evaluate whether Postconditioning (ischemic or with ciclosporin-A (CsA)) could reduce ischemia-reperfusion injury in a cardiac arrest model when applied at the start of reperfusion or after a delay. An isolated rat heart model was used as a model of DCD. Hearts were submitted to a cardiac arrest of 40 min of global warm ischemia (37 °C) followed by 3 h of 4 °C-cold preservation, then 60 min reperfusion. Hearts were randomly allocated into the following groups: control, ischemic postconditioning (POST, consisting of two episodes each of 30 s ischemia and 30 s reperfusion at the onset of reperfusion), and CsA group (CsA was perfused at 250 nM for 10 min at reperfusion). In respective subgroups, POST and CsA were applied after a delay of 3, 10, and 20 min. Necrosis was lower in CsA and POST versus controls (p < 0.01) whereas heart functions were improved (p < 0.01). However, while the POST lost its efficacy if delayed beyond 3 min of reperfusion, CsA treatment surprisingly showed a reduction of necrosis even if applied after a delay of 3 and 10 min of reperfusion (p < 0.01). This cardioprotection by delayed CsA application correlated with better functional recovery and higher mitochondrial respiratory index. Furthermore, calcium overload necessary to induce mitochondrial permeability transition pore (MPTP) opening was similar in all cardioprotection groups, suggesting a crucial role of MPTP in this delayed protection of DCD hearts.
Keywords: ciclosporin A-postconditioning–ischemia reperfusion injury (IRI)-delayed reperfusion-mitochondria-permeability transition pore; donation after circulatory death (DCD); heart transplantation.
Conflict of interest statement
All authors have no conflict of interest to disclose.
Figures





References
-
- Suarez-Pierre A., Iguidbashian J., Stuart C., King R.W., Cotton J., Carroll A.M., Cleveland J.C., Fullerton D.A., Pal J.D. Appraisal of Donation After Circulatory Death: How Far Could We Expand the Heart Donor Pool? Ann. Thorac. Surg. 2022;114:676–682. doi: 10.1016/j.athoracsur.2022.01.042. - DOI - PubMed
-
- Dhital K.K., Iyer A., Connellan M., Chew H.C., Gao L., Doyle A., Hicks M., Kumarasinghe G., Soto C., Dinale A., et al. Adult heart transplantation with distant procurement and ex-vivo preservation of donor hearts after circulatory death: A case series. Lancet. 2015;385:2585–2591. doi: 10.1016/S0140-6736(15)60038-1. - DOI - PubMed
-
- Schirone L., Forte M., D’Ambrosio L., Valenti V., Vecchio D., Schiavon S., Spinosa G., Sarto G., Petrozza V., Frati G., et al. An Overview of the Molecular Mechanisms Associated with Myocardial Ischemic Injury: State of the Art and Translational Perspectives. Cells. 2022;11:1165. doi: 10.3390/cells11071165. - DOI - PMC - PubMed
-
- Sanz M.N., Farine E., Niederberger P., Méndez-Carmona N., Wyss R.K., Arnold M., Gulac P., Fiedler G.M., Gressette M., Garnier A., et al. Cardioprotective reperfusion strategies differentially affect mitochondria: Studies in an isolated rat heart model of donation after circulatory death (DCD) Am. J. Transplant. 2019;19:331–344. doi: 10.1111/ajt.15024. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
