

The Role of Inflammation in Cardiovascular Disease
- PMID: 36361701
- PMCID: PMC9658900
- DOI: 10.3390/ijms232112906
The Role of Inflammation in Cardiovascular Disease
Abstract
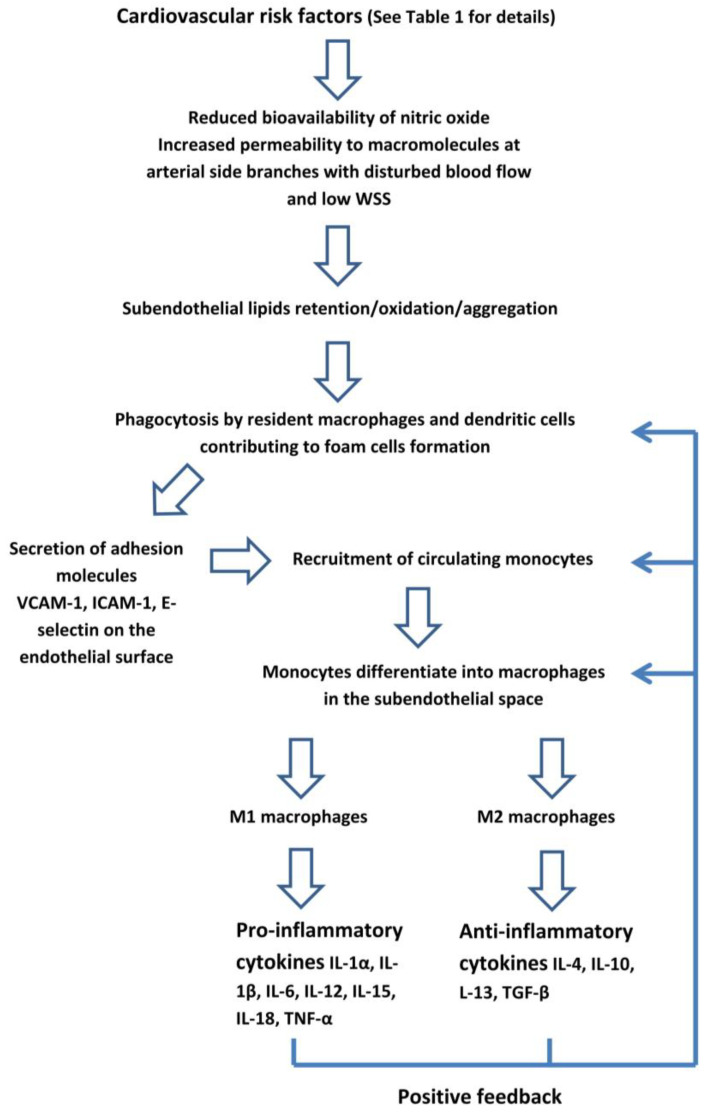
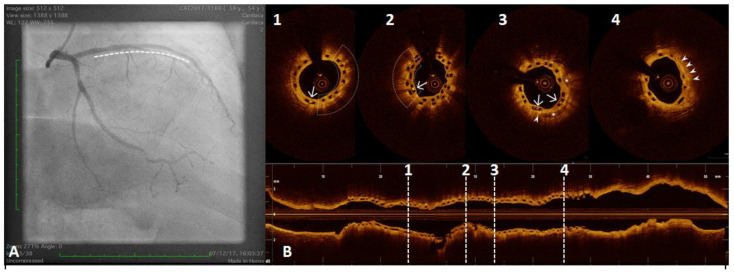
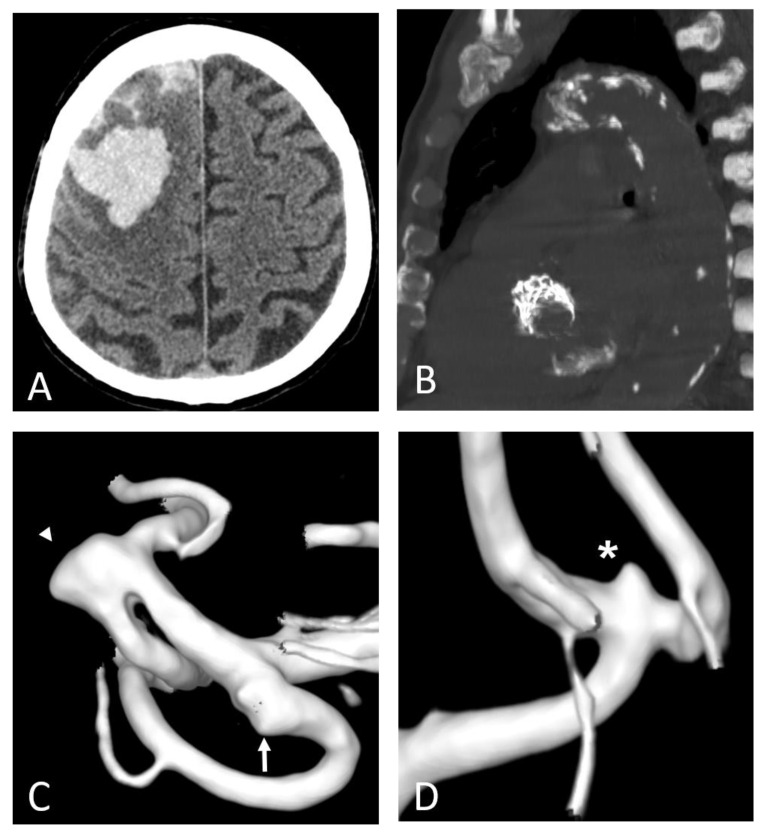
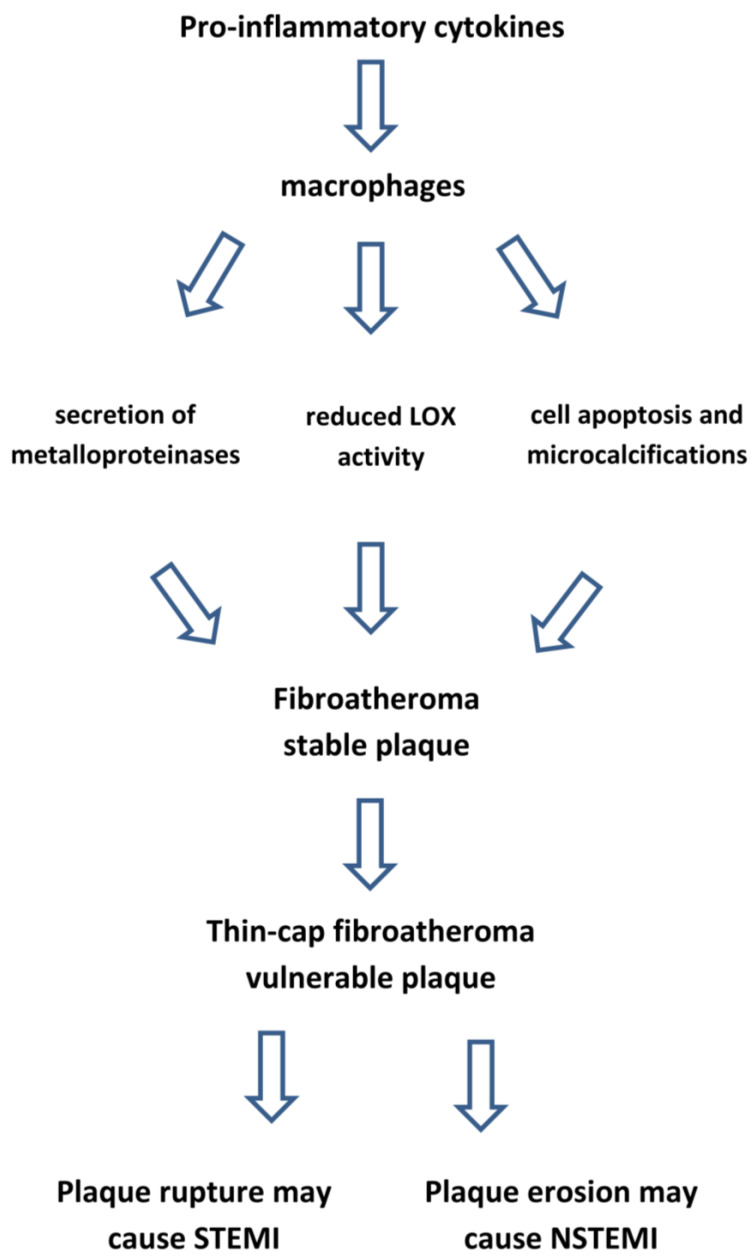
Atherosclerosis is a chronic inflammatory disease, in which the immune system has a prominent role in its development and progression. Inflammation-induced endothelial dysfunction results in an increased permeability to lipoproteins and their subendothelial accumulation, leukocyte recruitment, and platelets activation. Recruited monocytes differentiate into macrophages which develop pro- or anti-inflammatory properties according to their microenvironment. Atheroma progression or healing is determined by the balance between these functional phenotypes. Macrophages and smooth muscle cells secrete inflammatory cytokines including interleukins IL-1β, IL-12, and IL-6. Within the arterial wall, low-density lipoprotein cholesterol undergoes an oxidation. Additionally, triglyceride-rich lipoproteins and remnant lipoproteins exert pro-inflammatory effects. Macrophages catabolize the oxidized lipoproteins and coalesce into a lipid-rich necrotic core, encapsulated by a collagen fibrous cap, leading to the formation of fibro-atheroma. In the conditions of chronic inflammation, macrophages exert a catabolic effect on the fibrous cap, resulting in a thin-cap fibro-atheroma which makes the plaque vulnerable. However, their morphology may change over time, shifting from high-risk lesions to more stable calcified plaques. In addition to conventional cardiovascular risk factors, an exposure to acute and chronic psychological stress may increase the risk of cardiovascular disease through inflammation mediated by an increased sympathetic output which results in the release of inflammatory cytokines. Inflammation is also the link between ageing and cardiovascular disease through increased clones of leukocytes in peripheral blood. Anti-inflammatory interventions specifically blocking the cytokine pathways reduce the risk of myocardial infarction and stroke, although they increase the risk of infections.
Keywords: atherosclerosis; cerebral artery aneurysm; coronary artery disease; coronary atherosclerotic plaque; inflammation; stroke.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
