

Application and Impact of Antiviral Therapy for Patients with HBV-Related Hepatocellular Carcinoma Receiving Sorafenib and Lenvatinib Treatment
- PMID: 36366452
- PMCID: PMC9692815
- DOI: 10.3390/v14112355
Application and Impact of Antiviral Therapy for Patients with HBV-Related Hepatocellular Carcinoma Receiving Sorafenib and Lenvatinib Treatment
Abstract
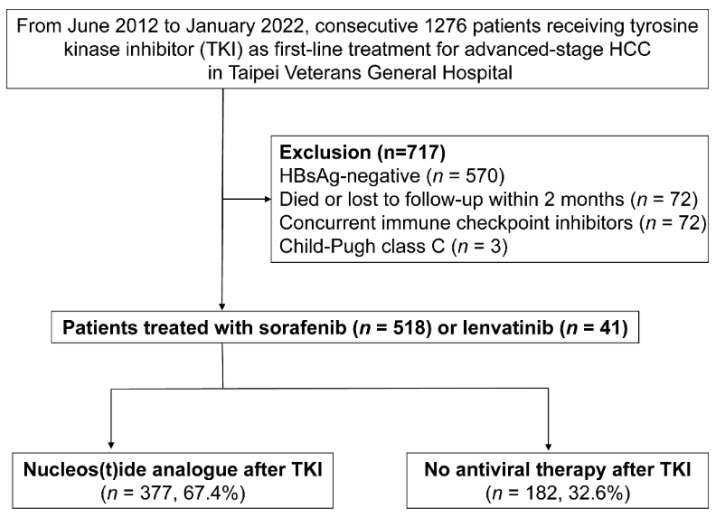
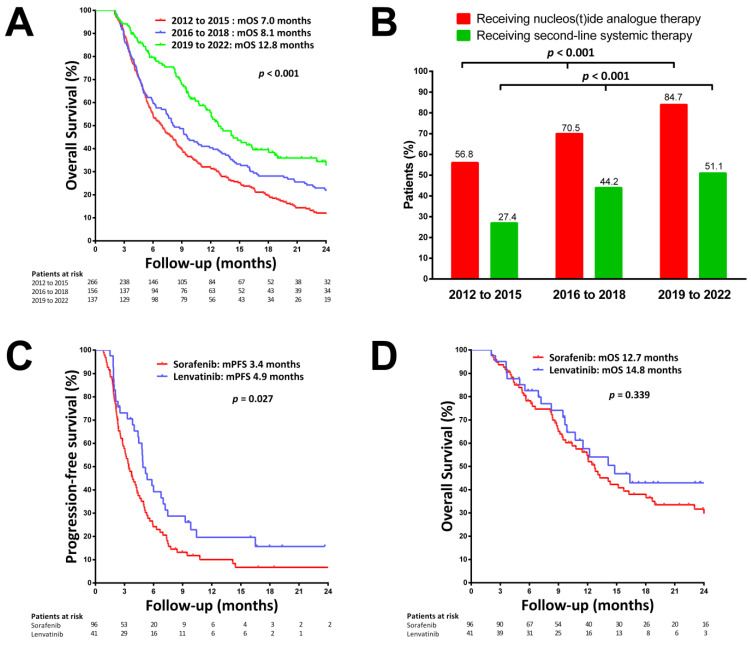
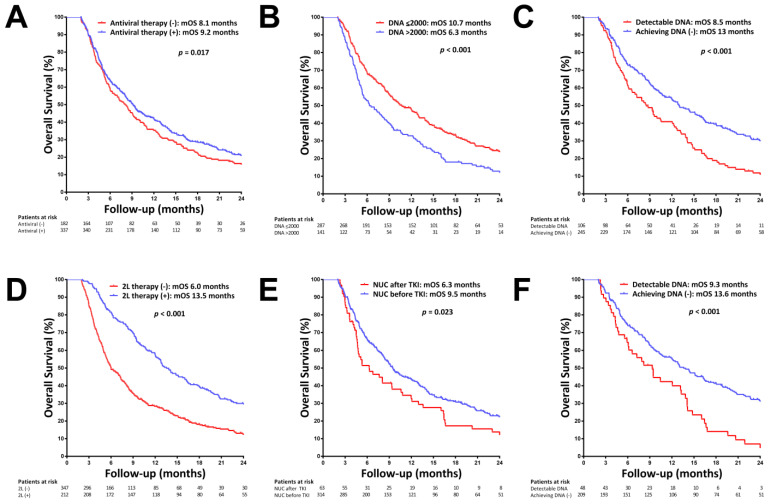
Overall survival (OS) in patients with advanced hepatocellular carcinoma (HCC) has improved in the era of multi-line sequential therapy. The application of antiviral therapy and its impact on survival for patients with HBV-related HCC needs to be reassessed. The aim of this study was to evaluate the application and impact of antiviral therapy on survival for patients with HBV-related HCC receiving tyrosine kinase inhibitor (TKI) therapy. Patients with advanced HBV-related HCC treated with sorafenib or lenvatinib as first-line therapy with (n = 377) and without (n = 182) nucleos(t)ide analogue (NUC) therapy were retrospectively enrolled. Prognostic factors of OS were evaluated. Secular trends in the increased application of NUC therapy and improved survival were observed in the last decade. The HBV reactivation rate in patients without NUC therapy was 6.6%. By multivariate analysis, baseline low HBV viral load, achieving undetectable HBV DNA after TKI therapy, and ability to receive second-line therapy were found to be independent predictors of OS. In subgroup patients with NUC therapy, starting NUC before TKI was associated with a better OS. In conclusion, the application of antiviral therapy for patients with HBV-related HCC receiving TKI therapy has increased over time. Achieving complete virological suppression may contribute to a better OS in patients with advanced HBV-related HCC.
Keywords: antiviral therapy; entecavir; hepatitis B virus; hepatocellular carcinoma; lenvatinib; sorafenib; tenofovir; tyrosine kinase inhibitor.
Conflict of interest statement
Y.-H.H. has received research grants from Gilead Sciences and Bristol-Meyers Squibb, and honoraria from Abbvie, Gilead Sciences, Bristol-Meyers Squibb, Ono Pharmaceutical, Merck Sharp & Dohme, Eisai, Eli Lilly, Ipsen, and Roche and has served in an advisory role for Abbvie, Gilead Sciences, Bristol-Meyers Squibb, Ono Pharmaceuticals, Eisai, Eli Lilly, Ipsen, Merck Sharp & Dohme, and Roche. I.-C.L. has received honoraria from Gilead Sciences, Bristol-Meyers Squibb, Abbvie, Merck Sharp & Dohme, Bayer, Eisai, Ipsen, and Roche and has served in an advisory role for Gilead Sciences. The other authors declare no conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
