

Estimated Monetary Value of Future Research Clarifying Uncertainties Around the Optimal Adult Hearing Screening Schedule
- PMID: 36367737
- PMCID: PMC9652748
- DOI: 10.1001/jamahealthforum.2022.4065
Estimated Monetary Value of Future Research Clarifying Uncertainties Around the Optimal Adult Hearing Screening Schedule
Abstract
Importance: Adult hearing screening is not routinely performed, and most individuals with hearing loss (HL) have never had their hearing tested as adults.
Objective: To project the monetary value of future research clarifying uncertainties around the optimal adult hearing screening schedule.
Design, setting, and participants: In this economic evaluation, a validated decision model of HL (DeciBHAL-US: Decision model of the Burden of Hearing loss Across the Lifespan) was used to simulate current detection and treatment of HL vs hearing screening schedules. Key model inputs included HL incidence (0.06%-10.42%/y), hearing aid uptake (0.54%-8.14%/y), screening effectiveness (1.62 × hearing aid uptake), utility benefits of hearing aids (+0.11), and hearing aid device costs ($3690). Distributions to model parameters for probabilistic uncertainty analysis were assigned. The expected value of perfect information (EVPI) and expected value of partial perfect information (EVPPI) using a willingness to pay of $100 000 per quality-adjusted life-year (QALY) was estimated. The EVPI and EVPPI estimate the upper bound of the dollar value of future research. This study was based on 40-year-old persons over their remaining lifetimes in a US primary care setting.
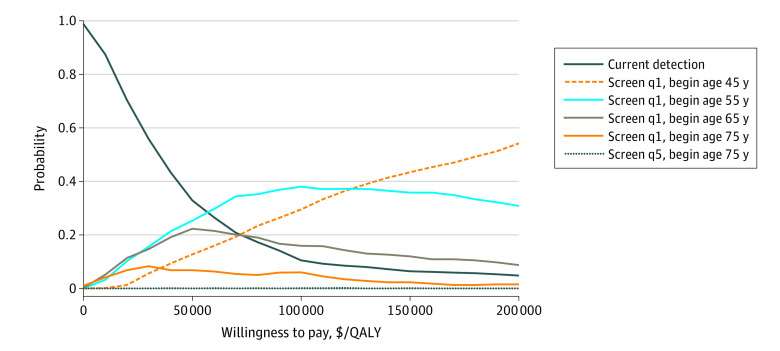
Exposures: Screening schedules beginning at ages 45, 55, 65, and 75 years, and frequencies of every 1 or 5 years.
Main outcomes and measures: The main outcomes were QALYs and costs (2020 US dollars) from a health system perspective.
Results: The average incremental cost-effectiveness ratio for yearly screening beginning at ages 55 to 75 years ranged from $39 200 to $80 200/QALY. Yearly screening beginning at age 55 years was the optimal screening schedule in 38% of probabilistic uncertainty analysis simulations. The population EVPI, or value of reducing all uncertainty, was $8.2 to $12.6 billion varying with willingness to pay and the EVPPI, or value of reducing all screening effectiveness uncertainty, was $2.4 billion.
Conclusions and relevance: In this economic evaluation of US adult hearing screening, large uncertainty around the optimal adult hearing screening schedule was identified. Future research on hearing screening has a high potential value so is likely justified.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
