

Intestinal toxicity to CTLA-4 blockade driven by IL-6 and myeloid infiltration
- PMID: 36367776
- PMCID: PMC9664499
- DOI: 10.1084/jem.20221333
Intestinal toxicity to CTLA-4 blockade driven by IL-6 and myeloid infiltration
Abstract
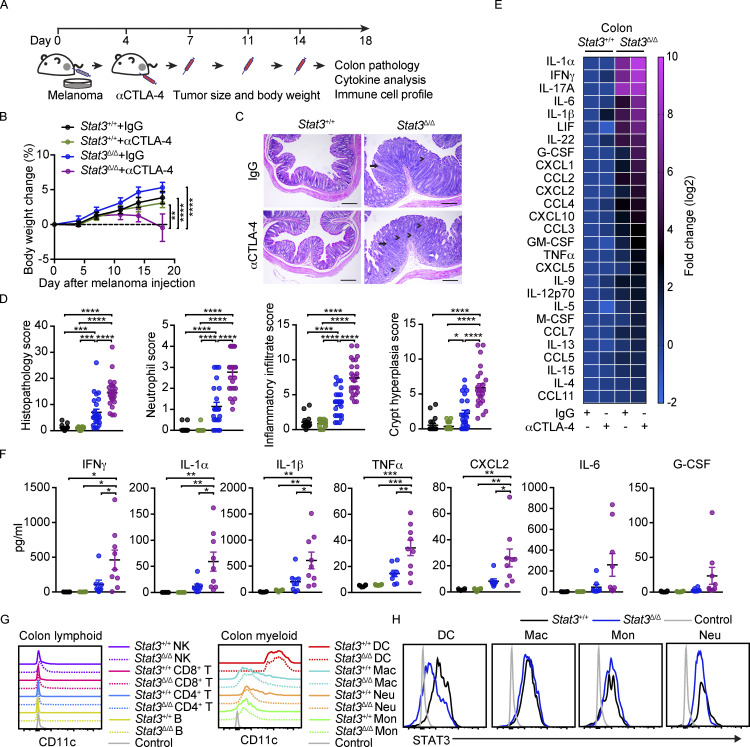
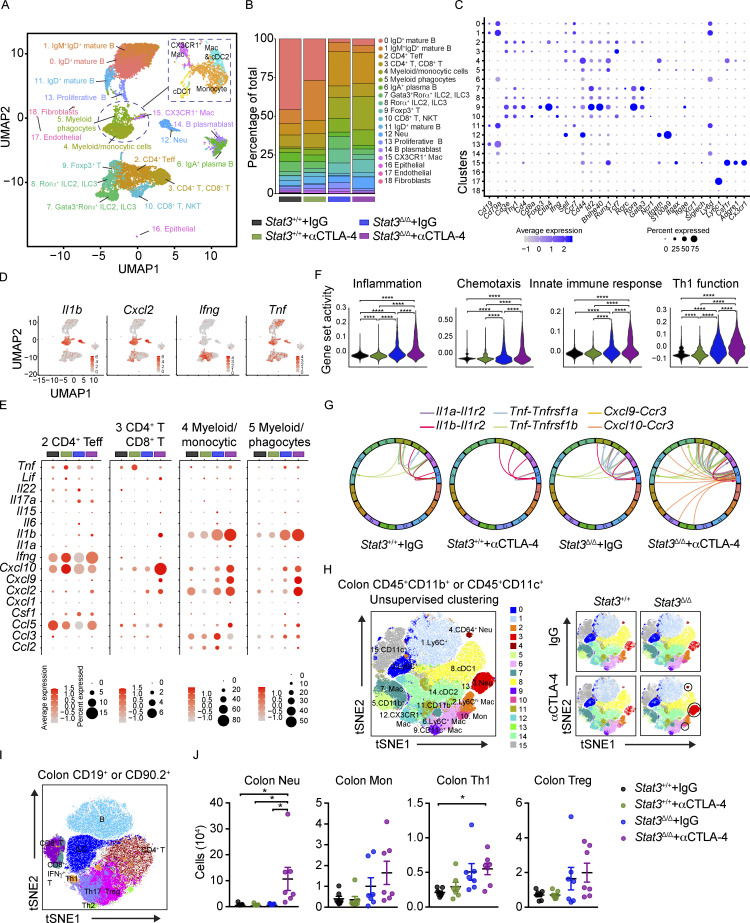
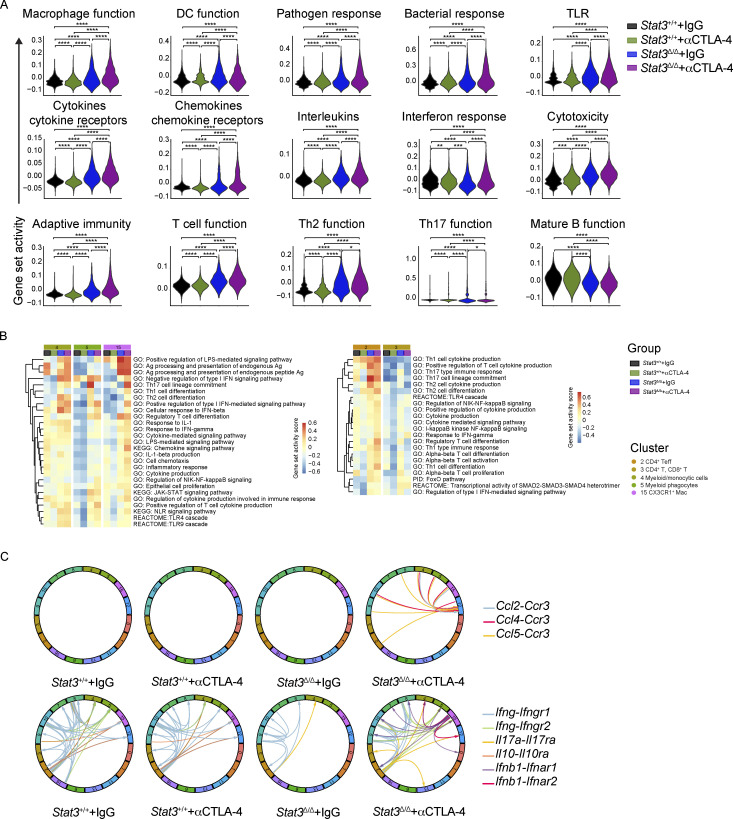
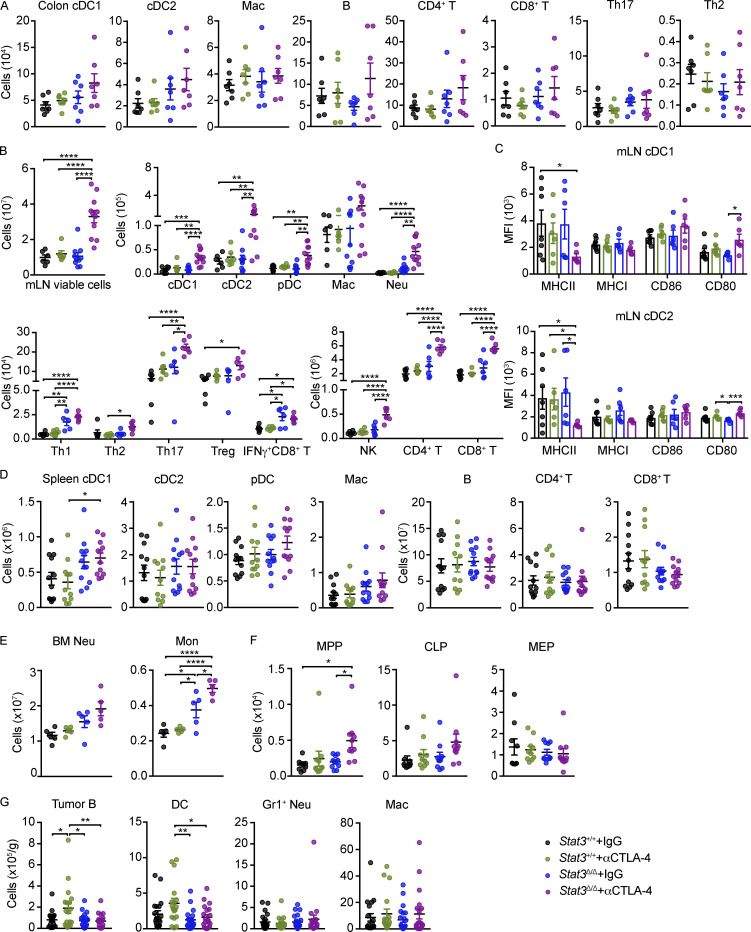
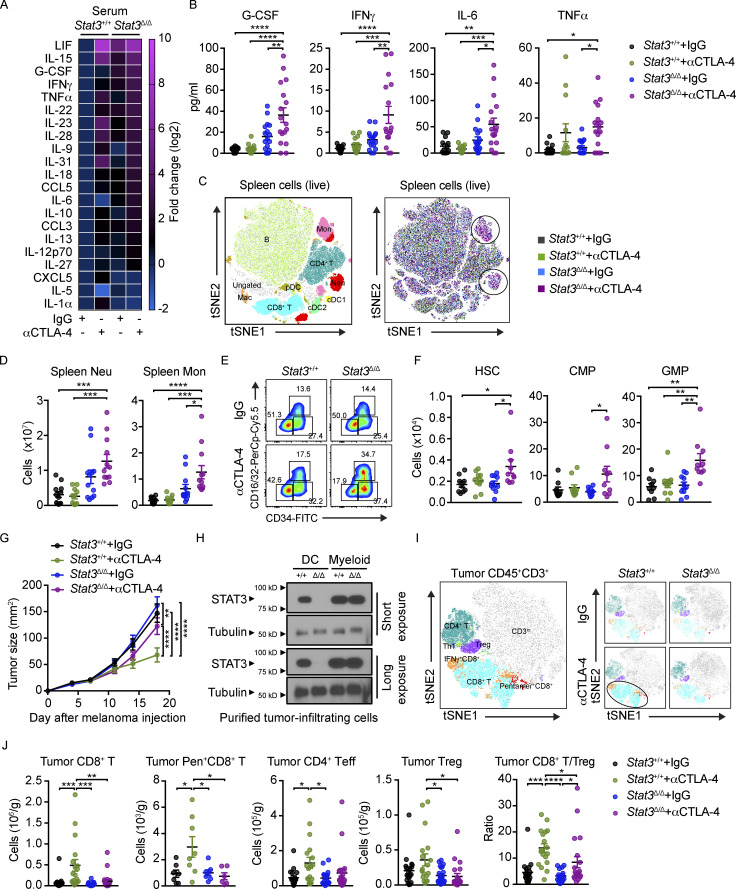
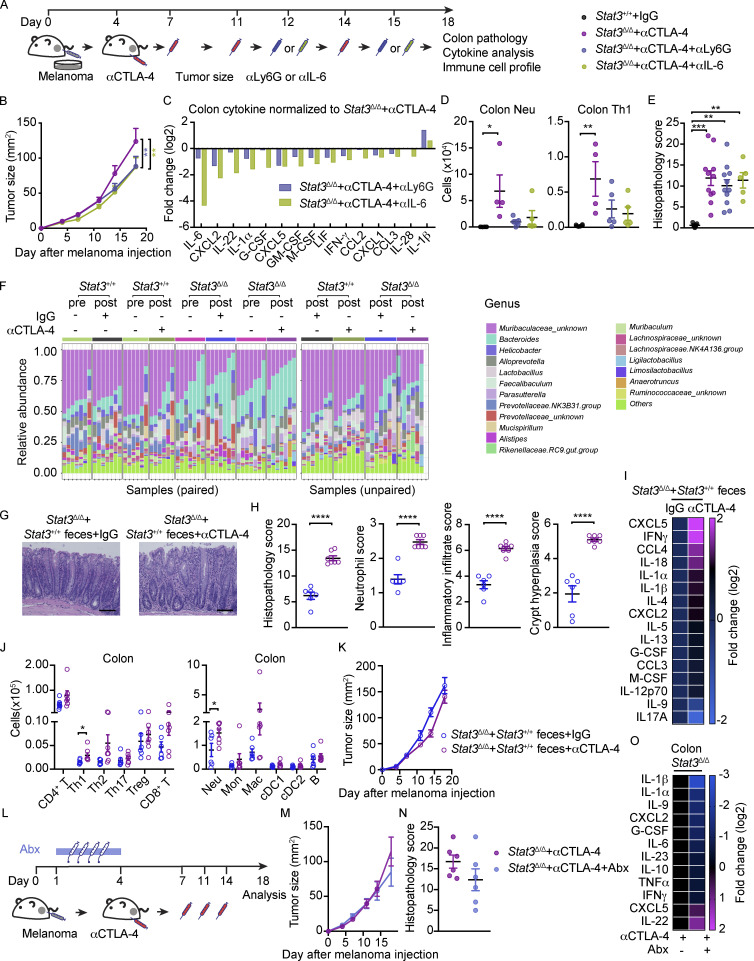
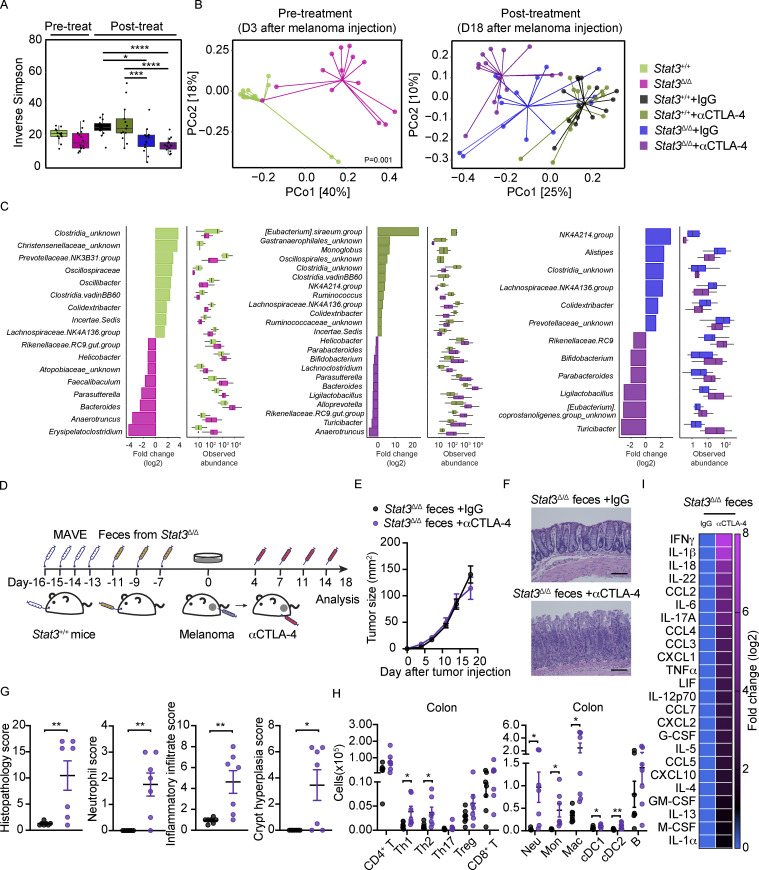
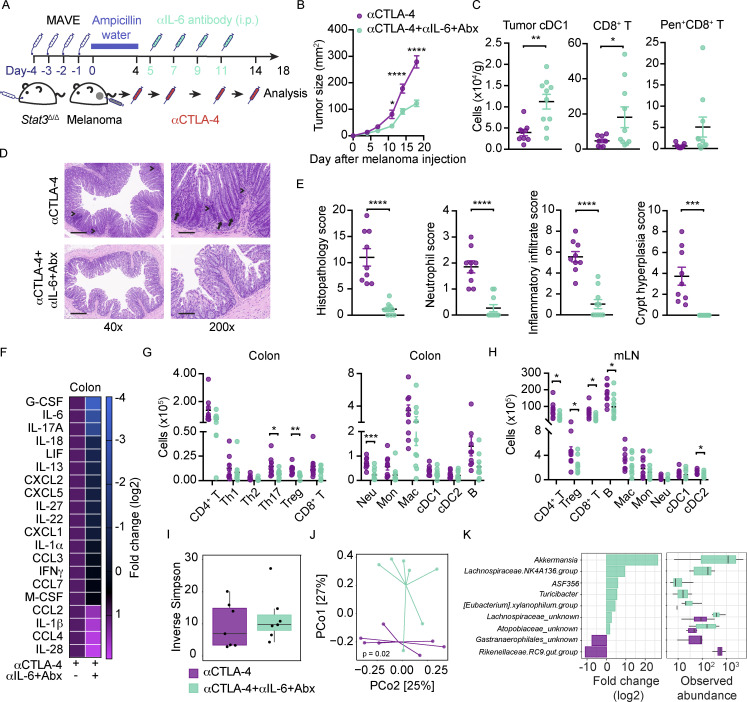
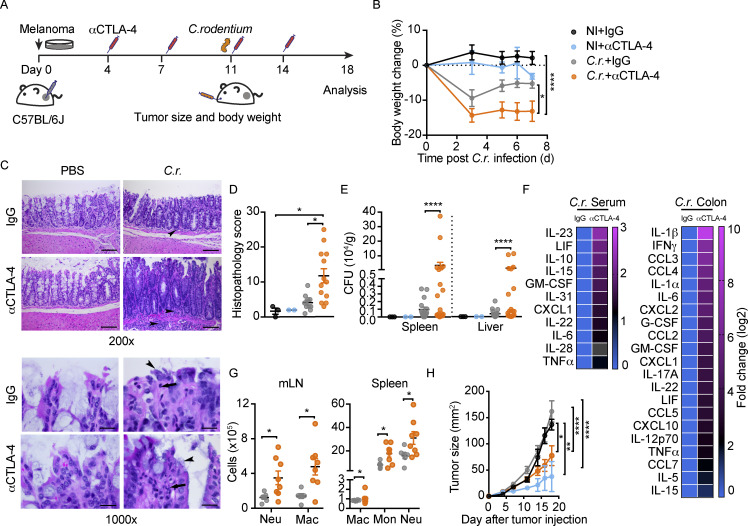
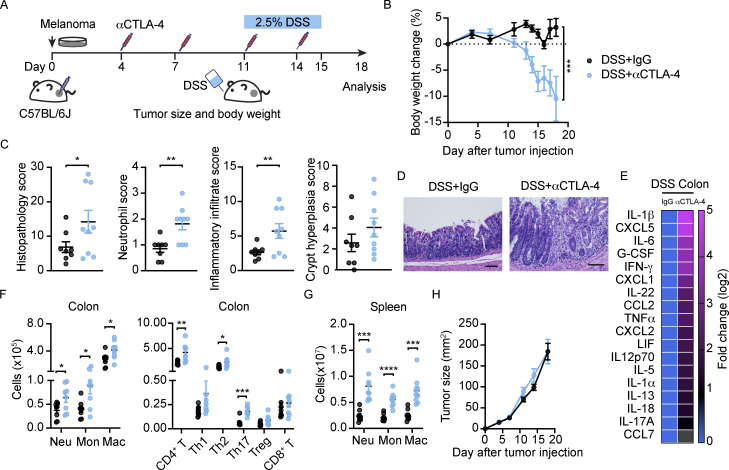
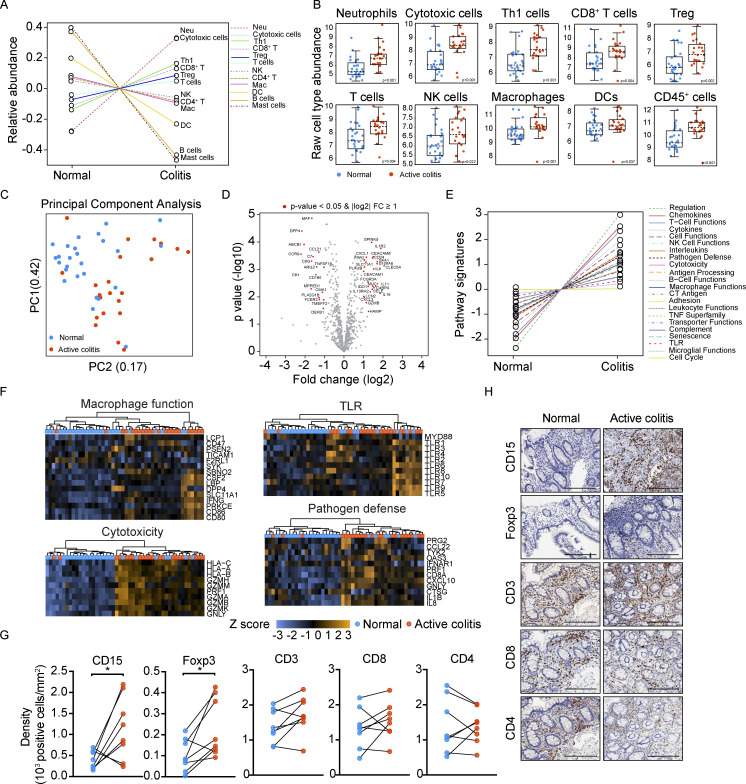
Immune checkpoint blockade (ICB) has revolutionized cancer treatment, yet quality of life and continuation of therapy can be constrained by immune-related adverse events (irAEs). Limited understanding of irAE mechanisms hampers development of approaches to mitigate their damage. To address this, we examined whether mice gained sensitivity to anti-CTLA-4 (αCTLA-4)-mediated toxicity upon disruption of gut homeostatic immunity. We found αCTLA-4 drove increased inflammation and colonic tissue damage in mice with genetic predisposition to intestinal inflammation, acute gastrointestinal infection, transplantation with a dysbiotic fecal microbiome, or dextran sodium sulfate administration. We identified an immune signature of αCTLA-4-mediated irAEs, including colonic neutrophil accumulation and systemic interleukin-6 (IL-6) release. IL-6 blockade combined with antibiotic treatment reduced intestinal damage and improved αCTLA-4 therapeutic efficacy in inflammation-prone mice. Intestinal immune signatures were validated in biopsies from patients with ICB colitis. Our work provides new preclinical models of αCTLA-4 intestinal irAEs, mechanistic insights into irAE development, and potential approaches to enhance ICB efficacy while mitigating irAEs.
© 2022 Zhou et al.
Conflict of interest statement
Disclosures: A.P. Cogdill reported “other” from Immunai, Vastbiome, and Daiichi Sankyo outside the submitted work. D.H. Johnson reported personal fees from Bristol Meyers Squibb, AstraZeneca, Nektar Therapeutics, Pfizer, Brightpath Therapeutics, and Sanofi-Regeneron outside the submitted work. W. Peng reported personal fees from Fresh Wind Biotechnologies outside the submitted work. M. Tetzlaff reported personal fees from Myriad Genetics outside the submitted work. M.M. Gubin reported a personal honorarium of $1,000.00 USD per year from Springer Nature Ltd. for serving as an associate editor for the journal
Figures
References
-
- Abu-Sbeih, H., Faleck D.M., Ricciuti B., Mendelsohn R.B., Naqash A.R., Cohen J.V., Sellers M.C., Balaji A., Ben-Betzalel G., Hajir I., et al. . 2020. Immune checkpoint inhibitor therapy in patients with preexisting Inflammatory Bowel Disease. J. Clin. Oncol. 38:576–583. 10.1200/JCO.19.01674 - DOI - PMC - PubMed
-
- Andrews, M.C., Duong C.P.M., Gopalakrishnan V., Iebba V., Chen W.S., Derosa L., Khan M.A.W., Cogdill A.P., White M.G., Wong M.C., et al. . 2021. Gut microbiota signatures are associated with toxicity to combined CTLA-4 and PD-1 blockade. Nat. Med. 27:1432–1441. 10.1038/s41591-021-01406-6 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
