

Value of low-keV virtual monoenergetic plus dual-energy computed tomographic imaging for detection of acute pulmonary embolism
- PMID: 36367855
- PMCID: PMC9651561
- DOI: 10.1371/journal.pone.0277060
Value of low-keV virtual monoenergetic plus dual-energy computed tomographic imaging for detection of acute pulmonary embolism
Abstract
Objective: To compare diagnostic values between the 40 keV virtual monoenergetic plus (40 keV VMI+) dual source dual energy computed tomography (DSDECT) pulmonary angiography images and the standard mixed (90 and 150 kV) images for the detection of acute pulmonary embolism (PE).
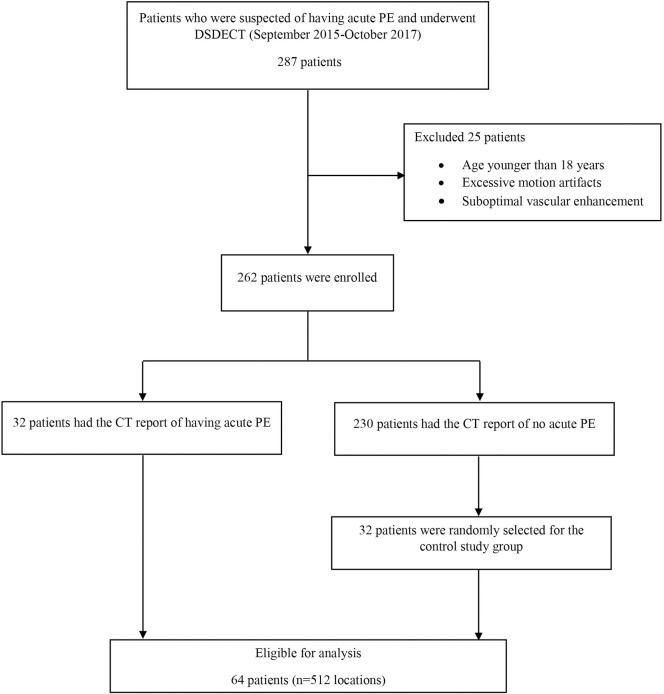
Methods: Chest DSDECTs of 64 patients who were suspected of having acute PE were retrospectively reviewed by two independent reviewers. The assessments of acute PE of all patients on a per-location basis were compared between the 40 keV VMI+ and the standard mixed datasets (reference standard) with a two-week interval.
Results: This study consisted of 64 patients (33 women and 31 men; mean age, 60.2 years; range 18-90 years), with a total of 512 locations. The interobserver agreement (Kappa) for detection of acute PE using the 40 keV VMI+ images and the standard mixed CT images were 0.7478 and 0.8750 respectively. The area under receiver operating characteristics (AuROC) for diagnosis of acute PE using the 40 keV VMI+ was 0.882. Four locations (0.78%) revealed a false negative result. Hypodense filling defects were identified in twelve locations (1.95%) in the 40 keV VMI+ images but had been interpreted as a negative study in the standard mixed CT images. The repeated reviews revealed that each location contained a hypodense filling defect but was overlooked on the standard mixed CT images.
Conclusions: Low-energy VMI + DSDECT images have beneficial in improving the diagnostic value of acute PE in doubtful or disregarded standard mixed images.
Copyright: © 2022 Wannasopha et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures




References
-
- Ruiz Y, Caballero P, Caniego JL, Friera A, Olivera MJ, Tagarro D, et al.. Prospective comparison of helical CT with angiography in pulmonary embolism: global and selective vascular territory analysis. Interobserver agreement. Eur Radiol. 2003;13(4):823–9. doi: 10.1007/s00330-002-1588-7 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
