

Radiofrequency Ablation Remodels the Tumor Microenvironment and Promotes Neutrophil-Mediated Abscopal Immunomodulation in Pancreatic Cancer
- PMID: 36367967
- PMCID: PMC9808367
- DOI: 10.1158/2326-6066.CIR-22-0379
Radiofrequency Ablation Remodels the Tumor Microenvironment and Promotes Neutrophil-Mediated Abscopal Immunomodulation in Pancreatic Cancer
Abstract
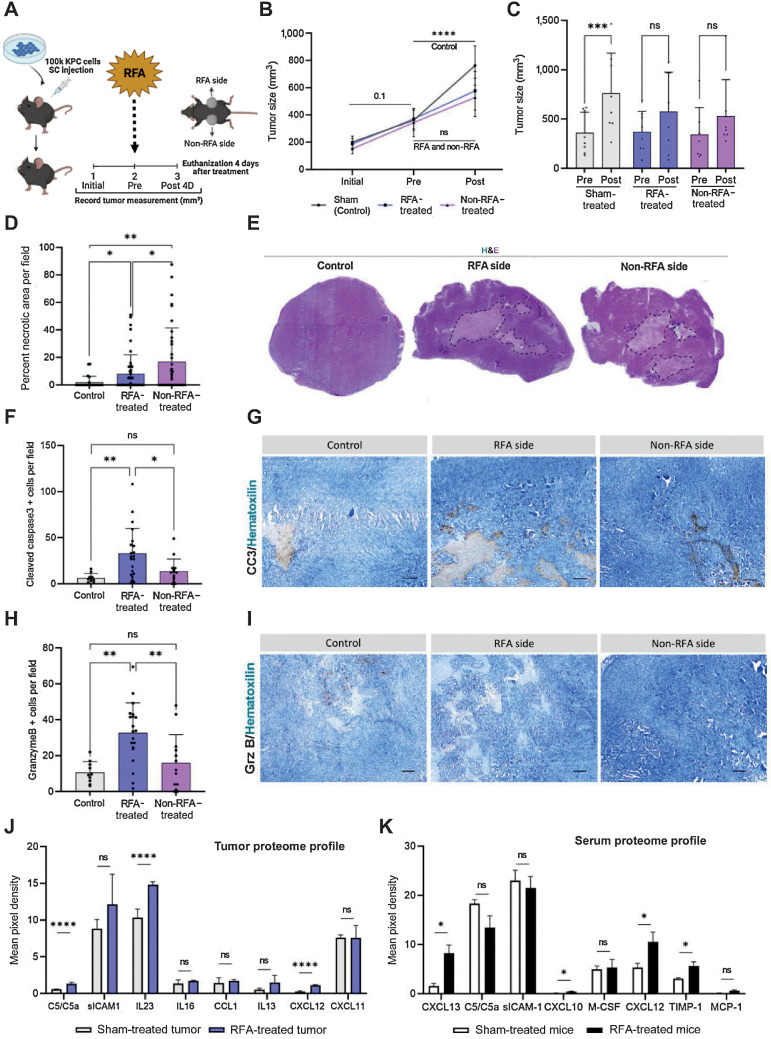
Pancreatic ductal adenocarcinoma (PDAC) presents a 5-year overall survival rate of 11%, despite efforts to improve clinical outcomes in the past two decades. Therapeutic resistance is a hallmark of this disease, due to its dense and suppressive tumor microenvironment (TME). Endoscopic ultrasound-guided radiofrequency ablation (EUS-RFA) is a promising local ablative and potential immunomodulatory therapy for PDAC. In this study, we performed RFA in a preclinical tumor-bearing KrasG12D; Trp53R172H/+; Pdx1:Cre (KPC) syngeneic model, analyzed local and abscopal affects after RFA and compared our findings with resected PDAC specimens. We found that RFA reduced PDAC tumor progression in vivo and promoted strong TME remodeling. In addition, we discovered tumor-infiltrating neutrophils determined abscopal effects. Using imaging mass cytometry, we showed that RFA elevated dendritic cell numbers in RFA-treated tumors and promoted a significant CD4+ and CD8+ T-cell abscopal response. In addition, RFA elevated levels of programmed death-ligand 1 (PD-L1) and checkpoint blockade inhibition targeting PD-L1 sustained tumor growth reduction in the context of RFA. This study indicates RFA treatment, which has been shown to increase tumor antigen shedding, promotes antitumor immunity. This is critical in PDAC where recent clinical immunotherapy trials have not resulted in substantial changes in overall survival.
©2022 The Authors; Published by the American Association for Cancer Research.
Figures



References
-
- Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM, Matrisian LM. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res 2014;74:2913–21. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
