

National Projections for Clinical Implications of Race-Free Creatinine-Based GFR Estimating Equations
- PMID: 36368777
- PMCID: PMC10103103
- DOI: 10.1681/ASN.2022070818
National Projections for Clinical Implications of Race-Free Creatinine-Based GFR Estimating Equations
Abstract
Background: The National Kidney Foundation and American Society of Nephrology Task Force on Reassessing the Inclusion of Race in Diagnosing Kidney Disease recently recommended a new race-free creatinine-based equation for eGFR. The effect on recommended clinical care across race and ethnicity groups is unknown.
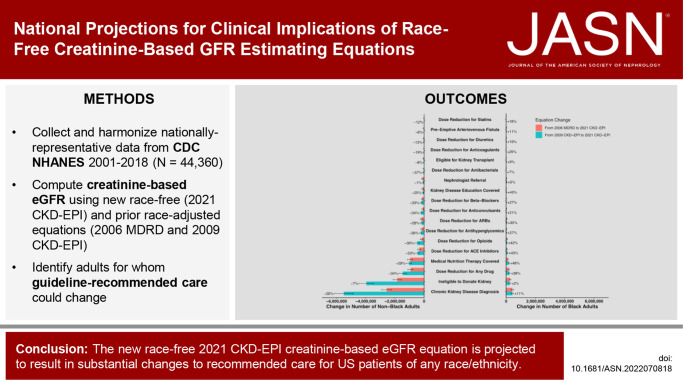
Methods: We analyzed nationally representative cross-sectional questionnaires and medical examinations from 44,360 participants collected between 2001 and 2018 by the National Health and Nutrition Examination Survey. We quantified the number and proportion of Black, White, Hispanic, and Asian/Other adults with guideline-recommended changes in care.
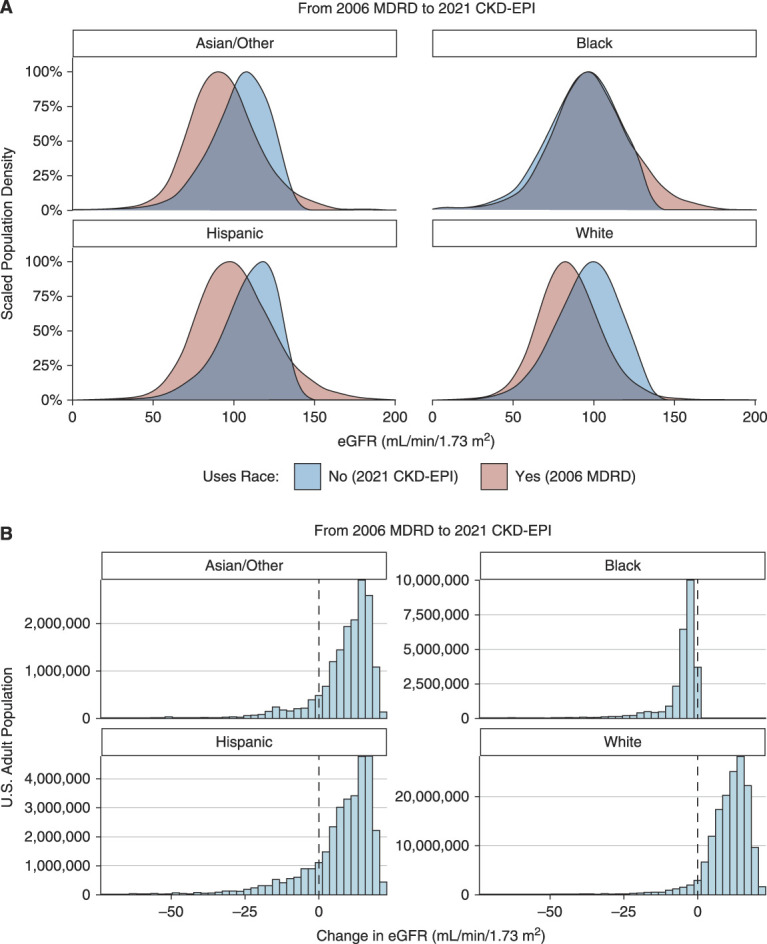
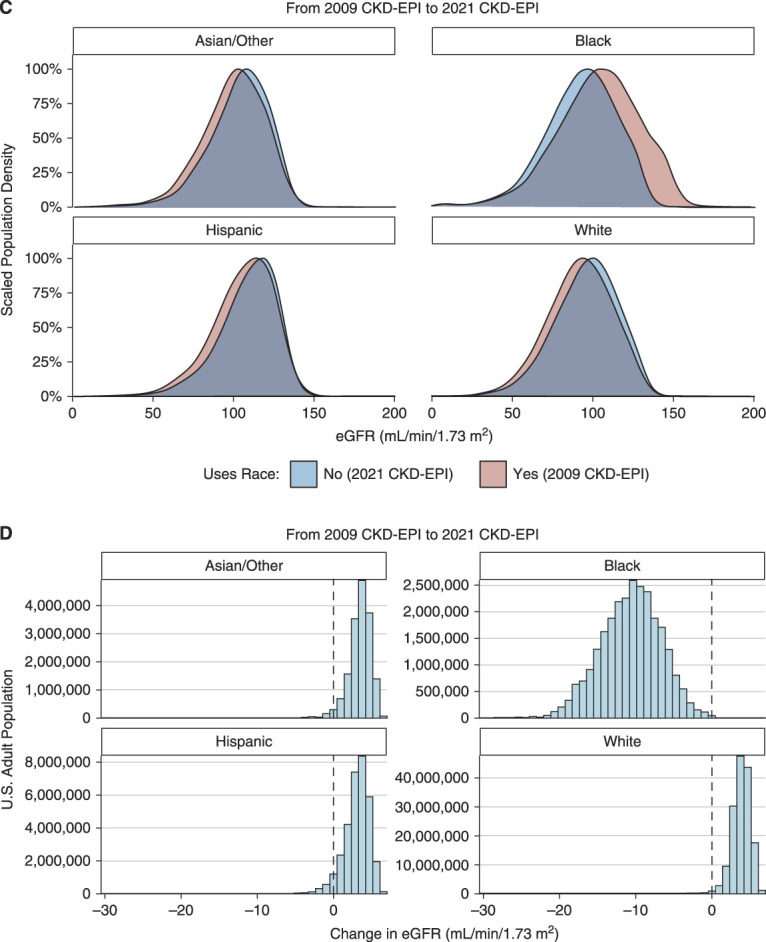
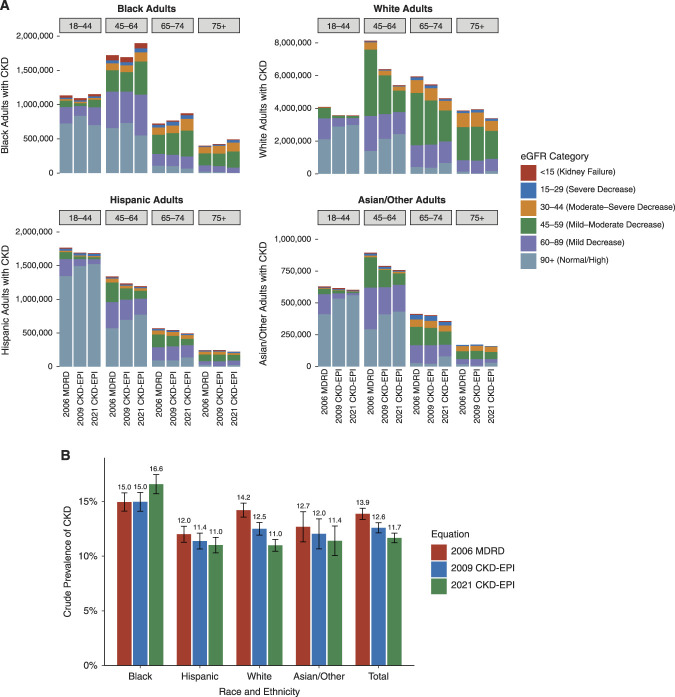
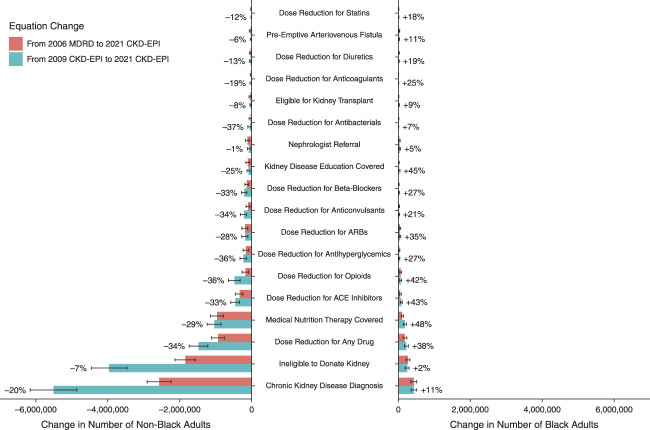
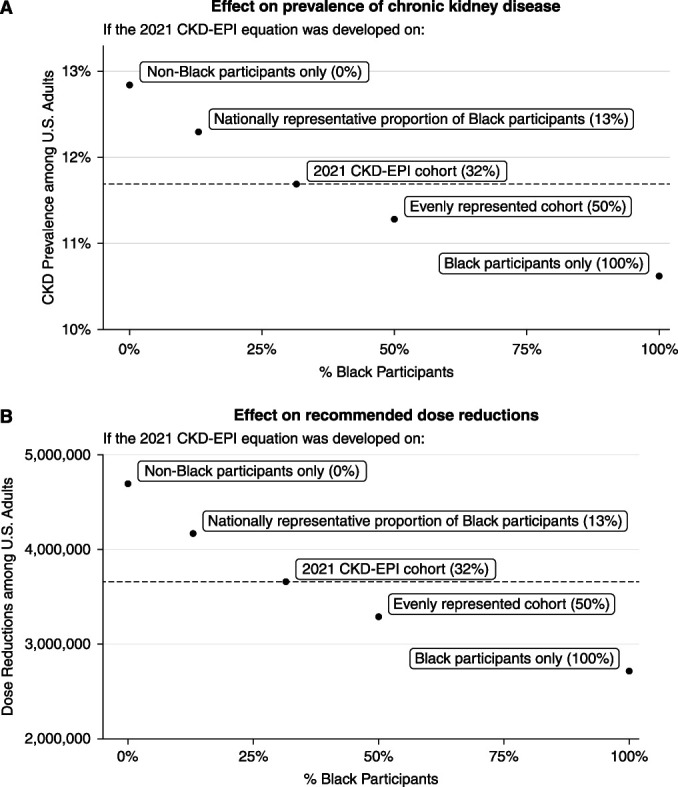
Results: The new equation, if applied nationally, could assign new CKD diagnoses to 434,000 (95% confidence interval [CI], 350,000 to 517,000) Black adults, reclassify 584,000 (95% CI, 508,000 to 667,000) to more advanced stages of CKD, restrict kidney donation eligibility for 246,000 (95% CI, 189,000 to 303,000), expand nephrologist referrals for 41,800 (95% CI, 19,800 to 63,800), and reduce medication dosing for 222,000 (95% CI, 169,000 to 275,000). Among non-Black adults, these changes may undo CKD diagnoses for 5.51 million (95% CI, 4.86 million to 6.16 million), reclassify 4.59 million (95% CI, 4.28 million to 4.92 million) to less advanced stages of CKD, expand kidney donation eligibility for 3.96 million (95% CI, 3.46 million to 4.46 million), reverse nephrologist referral for 75,800 (95% CI, 35,400 to 116,000), and reverse medication dose reductions for 1.47 million (95% CI, 1.22 million to 1.73 million). The racial and ethnic mix of the populations used to develop eGFR equations has a substantial effect on potential care changes.
Conclusion: The newly recommended 2021 CKD-EPI creatinine-based eGFR equation may result in substantial changes to recommended care for US patients of all racial and ethnic groups.
Copyright © 2022 by the American Society of Nephrology.
Conflict of interest statement
A.S. Levey reports receiving research funding from grants and contracts paid to Tufts Medical Center from NIH and NKF; reports contracts to paid from AstraZeneca (Data and Safety Monitoring Board (DSMB) for dapagliflozin trials); and reports receiving honoraria from academic medical centers for visiting professorships. H.A. Taylor reports having consultancy agreements with Pfizer, Novartis, and United Health Group (UHG); reports receiving research funding from 23andMe and UHG; and reports receiving honoraria from Pfizer, Novartis, and UHG. I.S. Kohane reports having consultancy agreements with Danaher; reports having an ownership interest in Activate Care, Canary Medical, and Inovalon; reports receiving honoraria from Janssen; and reports having an advisory or leadership role with Activate Care, Canary Medical, and Inovalon. J.K. Wang reports employment with PathAI; and having consultancy agreements with Prometheus Biosciences. L.A. Inker reports having consultancy agreements with Diamtrix; receiving research funding from to institute for research and contracts with the Chinnocks, NIH, NKF, Omeros, and Reata Pharmaceuticals; reports having consulting agreements with Tricida Inc.; reports having an advisory or leadership role with the Alport Foundation Medical Advisory Council and the NKF Scientific Advisory Board; and reports having other interests or relationships as an American Society of Nephrology member and an NKF member. N.R. Powe reports having an advisory or leadership role with Hennepin Health Care Research Institute, Patient Centered Outcomes Research Institute, Portland VA Research Foundation, Robert Wood Johnson Foundation, University of Washington, and Vanderbilt University. Because N.R. Powe is an associate editor of the
Figures
Comment in
-
GFR, Race, and Implications.J Am Soc Nephrol. 2023 Apr 1;34(4):721. doi: 10.1681/ASN.0000000000000096. J Am Soc Nephrol. 2023. PMID: 37000954 Free PMC article. No abstract available.
-
Author Reply: GFR, Race, and Implications.J Am Soc Nephrol. 2023 Apr 1;34(4):721-722. doi: 10.1681/ASN.0000000000000097. J Am Soc Nephrol. 2023. PMID: 37000955 Free PMC article. No abstract available.
References
-
- Eneanya ND, Yang W, Reese PP: Reconsidering the consequences of using race to estimate kidney function. JAMA 322: 113–114, 2019 - PubMed
-
- Vyas DA, Eisenstein LG, Jones DS: Hidden in plain sight - Reconsidering the use of race correction in clinical algorithms. N Engl J Med 383: 874–882, 2020 - PubMed
-
- Roberts DE: Abolish race correction. Lancet 397: 17–18, 2021 - PubMed
-
- Delgado C, Baweja M, Crews DC, Eneanya ND, Gadegbeku CA, Inker LA, et al. : A unifying approach for GFR estimation: Recommendations of the NKF-ASN Task Force on reassessing the inclusion of race in diagnosing kidney disease. Am J Kidney Dis 79: 268–288.e1, 2022 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
