

Outcomes and risks in palliative pancreatic surgery: an analysis of the German StuDoQ|Pancreas registry
- PMID: 36368993
- PMCID: PMC9652845
- DOI: 10.1186/s12893-022-01833-3
Outcomes and risks in palliative pancreatic surgery: an analysis of the German StuDoQ|Pancreas registry
Abstract
Background: Non-resectability is common in patients with pancreatic ductal adenocarcinoma (PDAC) due to local invasion or distant metastases. Then, biliary or gastroenteric bypasses or both are often established despite associated morbidity and mortality. The current study explores outcomes after palliative bypass surgery in patients with non-resectable PDAC.
Methods: From the prospectively maintained German StuDoQ|Pancreas registry, all patients with histopathologically confirmed PDAC who underwent non-resective pancreatic surgery between 2013 and 2018 were retrospectively identified, and the influence of the surgical procedure on morbidity and mortality was analyzed.
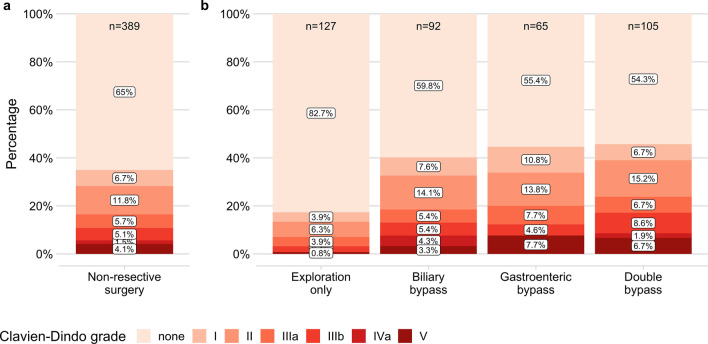
Results: Of 389 included patients, 127 (32.6%) underwent explorative surgery only, and a biliary, gastroenteric or double bypass was established in 92 (23.7%), 65 (16.7%) and 105 (27.0%). After exploration only, patients had a significantly shorter stay in the intensive care unit (mean 0.5 days [SD 1.7] vs. 1.9 [3.6], 2.0 [2.8] or 2.1 [2.8]; P < 0.0001) and in the hospital (median 7 days [IQR 4-11] vs. 12 [10-18], 12 [8-19] or 12 [9-17]; P < 0.0001), and complications occurred less frequently (22/127 [17.3%] vs. 37/92 [40.2%], 29/65 [44.6%] or 48/105 [45.7%]; P < 0.0001). In multivariable logistic regression, biliary stents were associated with less major (Clavien-Dindo grade ≥ IIIa) complications (OR 0.49 [95% CI 0.25-0.96], P = 0.037), whereas-compared to exploration only-biliary, gastroenteric, and double bypass were associated with more major complications (OR 3.58 [1.48-8.64], P = 0.005; 3.50 [1.39-8.81], P = 0.008; 4.96 [2.15-11.43], P < 0.001).
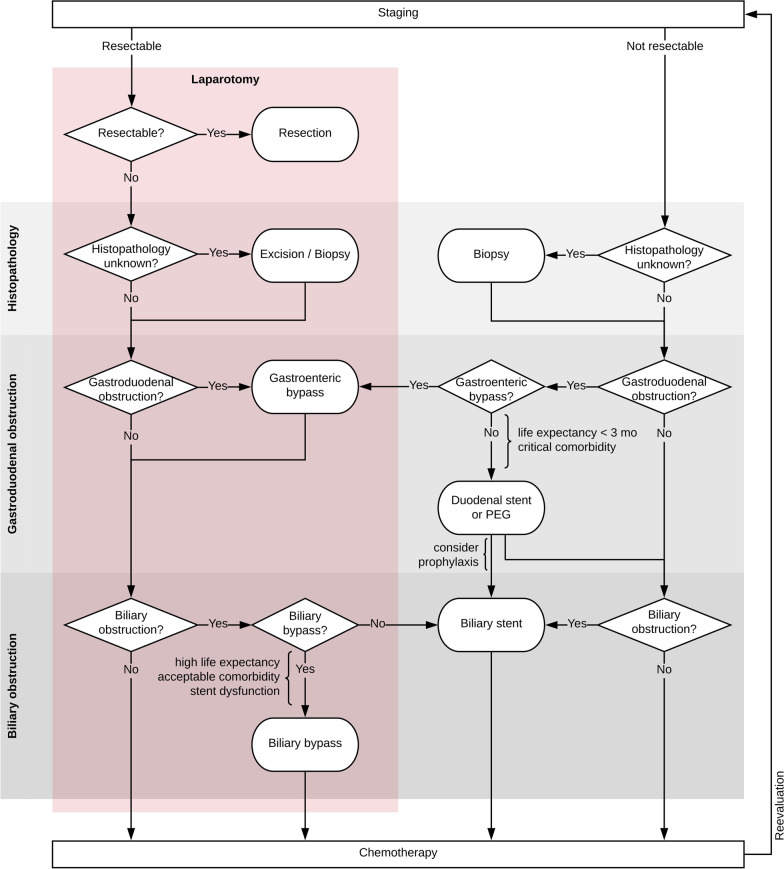
Conclusions: In patients with non-resectable PDAC, biliary, gastroenteric or double bypass surgery is associated with relevant morbidity and mortality. Although surgical palliation is indicated if interventional alternatives are inapplicable, or life expectancy is high, less invasive options should be considered.
Keywords: Biliary bypass; Explorative surgery; Gastroenteric bypass; Palliative surgery; Pancreatic ductal adenocarcinoma; Registry analysis.
© 2022. The Author(s).
Conflict of interest statement
FOH has received a research leave grant from the Bavarian Centre for Cancer Research (BZKF), partner site Munich, Germany. MW has received funding from the German Research Foundation (DFG, Grant #401299842). The remaining authors declare that they have no competing interests.
Figures


References
-
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. - PubMed
-
- Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM, Matrisian LM. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014;74(11):2913–2921. - PubMed
-
- Tempero MA, Malafa MP, Al-Hawary M, Asbun H, Behrman SW, Benson AB, et al. Pancreatic Adenocarcinoma, Version 1.2020, NCCN Clinical Practice Guidelines in Oncology: National Comprehensive Cancer Network NCCN; 2020. https://www.nccn.org/professionals/physician_gls/pdf/pancreatic.pdf. Accessed 26 Nov 2019.
-
- Ducreux M, Cuhna AS, Caramella C, Hollebecque A, Burtin P, Goere D, et al. Cancer of the pancreas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2015;26(Suppl 5):v56–68. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
