

The burden of rheumatoid arthritis in the Middle East and North Africa region, 1990-2019
- PMID: 36369238
- PMCID: PMC9652423
- DOI: 10.1038/s41598-022-22310-0
The burden of rheumatoid arthritis in the Middle East and North Africa region, 1990-2019
Abstract
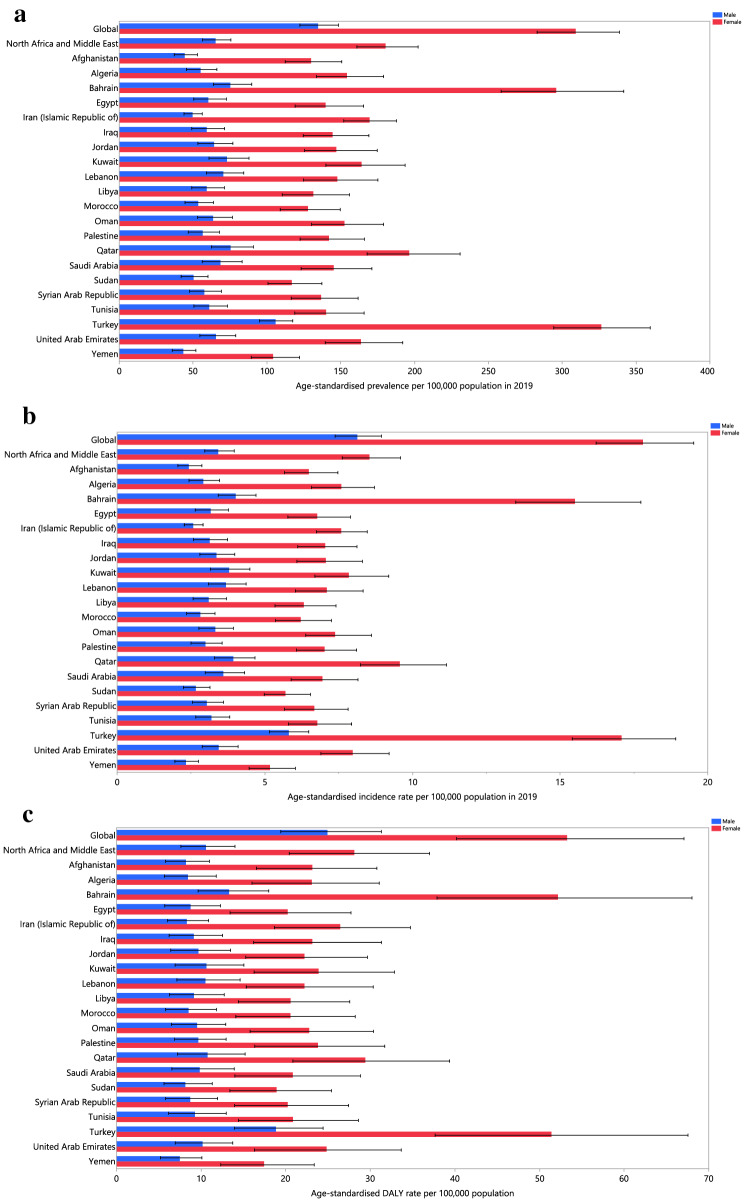
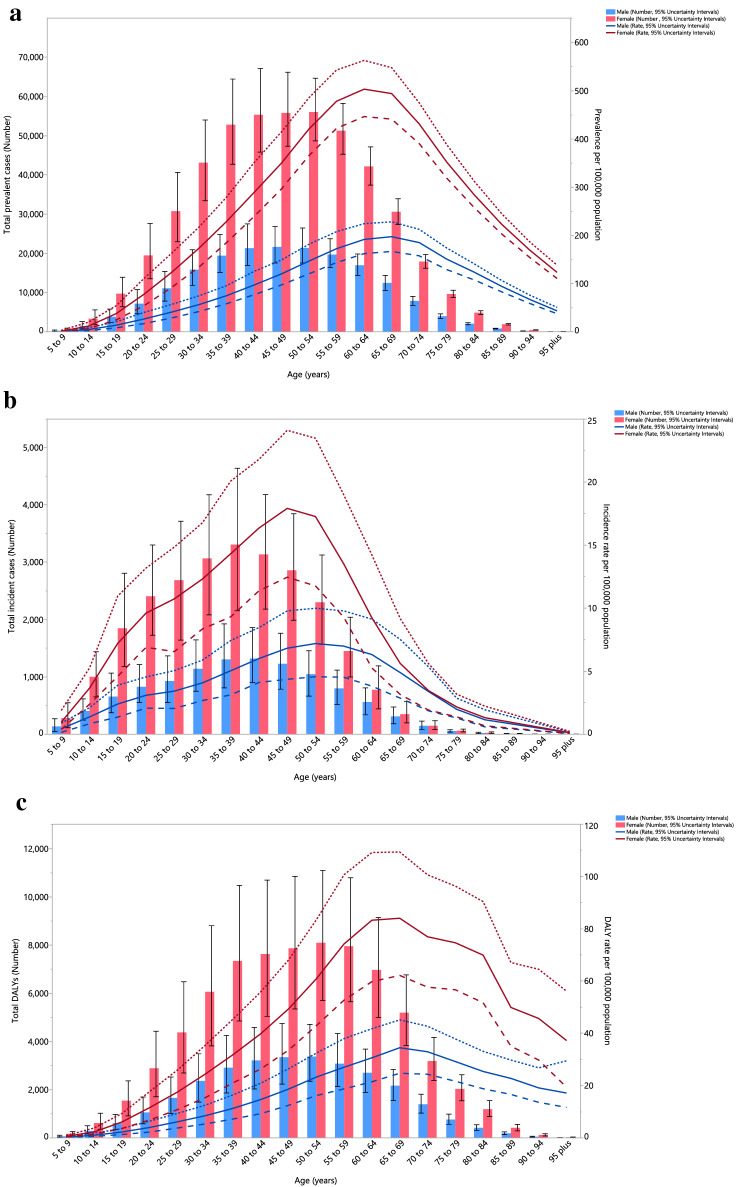
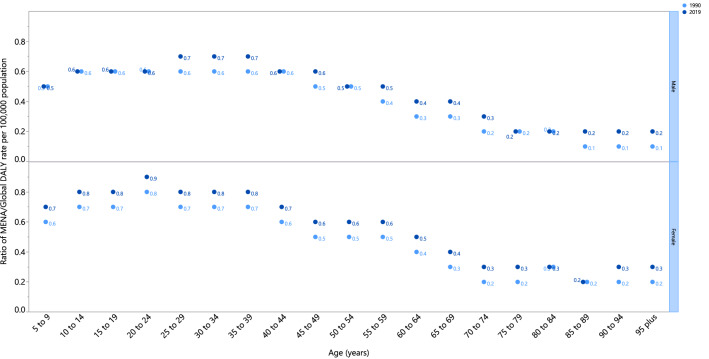
Rheumatoid arthritis (RA) is a chronic systemic autoimmune disease. The present study reported the burden of RA in the Middle East and North Africa (MENA) region from 1990 to 2019 by age, sex, and socio-demographic index (SDI). Publicly available data from the Global Burden of Disease (GBD) 2019 study was used to report the modelled point prevalence, annual incidence, and disability-adjusted life-years (DALYs) of RA, as counts and age-standardised rates with their corresponding 95% uncertainty intervals (UIs). In 2019, RA had an age-standardised point prevalence of 120.6 per 100,000 population (107.0-135.7) and an annual incidence rate of 5.9 (5.2-6.6) in MENA, which have increased 28.3% and 25.2%, respectively, since 1990. In 2019, the number of DALYs due to RA in the region was 103.6 thousand (74.2-136.7), with an age-standardised rate of 19.0 (13.9-24.9) DALYs per 100,000 population, which has increased by 18.6% since 1990 (6.7-28.2). The highest point prevalence was found in females aged 50-54, and in males aged 45-49. The highest number of DALYs was observed in the 50-54 age group. The MENA DALY rate was lower than the global rate (19.0 vs. 39.6 per 100,000), but the rate was higher in all age groups in 2019, when compared with 1990. In addition, from 1990 to 2019 an increased burden from RA was associated with an increase in SDI. In line with global trends, the burden of RA in the MENA region showed a steady increase from 1990 to 2019. This highlights the increasing need for updating the available health data to design more accurate guidelines to enable the early detection and treatment of RA in the MENA countries.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Khurana R, Berney SM. Clinical aspects of rheumatoid arthritis. Pathophysiology. 2005;12(3):153–165. - PubMed
-
- Scherer HU, Häupl T, Burmester GR. The etiology of rheumatoid arthritis. J. Autoimmun. 2020;110:102400. - PubMed
-
- Frisell T, Holmqvist M, Källberg H, Klareskog L, Alfredsson L, Askling J. Familial risks and heritability of rheumatoid arthritis: Role of rheumatoid factor/anti–citrullinated protein antibody status, number and type of affected relatives, sex, and age. Arthr. Rheum. 2013;65(11):2773–2782. - PubMed
-
- Sugiyama D, Nishimura K, Tamaki K, Tsuji G, Nakazawa T, Morinobu A, et al. Impact of smoking as a risk factor for developing rheumatoid arthritis: A meta-analysis of observational studies. Ann. Rheum. Dis. 2010;69(01):70. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
