

Complete mesocolic excision for right colonic cancer: prospective multicentre study
- PMID: 36369986
- PMCID: PMC10364501
- DOI: 10.1093/bjs/znac379
Complete mesocolic excision for right colonic cancer: prospective multicentre study
Abstract
Background: Complete mesocolic excision (CME) for right colonic cancer is a more complex operation than standard right hemicolectomy but evidence to support its routine use is still limited. This prospective multicentre study evaluated the effect of CME on long-term survival in colorectal cancer centres in Germany (RESECTAT trial). The primary hypothesis was that 5-year disease-free survival would be higher after CME than non-CME surgery. A secondary hypothesis was that there would be improved survival of patients with a mesenteric area greater than 15 000 mm2.
Methods: Centres were asked to continue their current surgical practices. The surgery was classified as CME if the superior mesenteric vein was dissected; otherwise it was assumed that no CME had been performed. All specimens were shipped to one institution for pathological analysis and documentation. Clinical data were recorded in an established registry for quality assurance. The primary endpoint was 5-year overall survival for stages I-III. Multivariable adjustment for group allocation was planned. Using a primary hypothesis of an increase in disease-free survival from 60 to 70 per cent, a sample size of 662 patients was calculated with a 50 per cent anticipated drop-out rate.
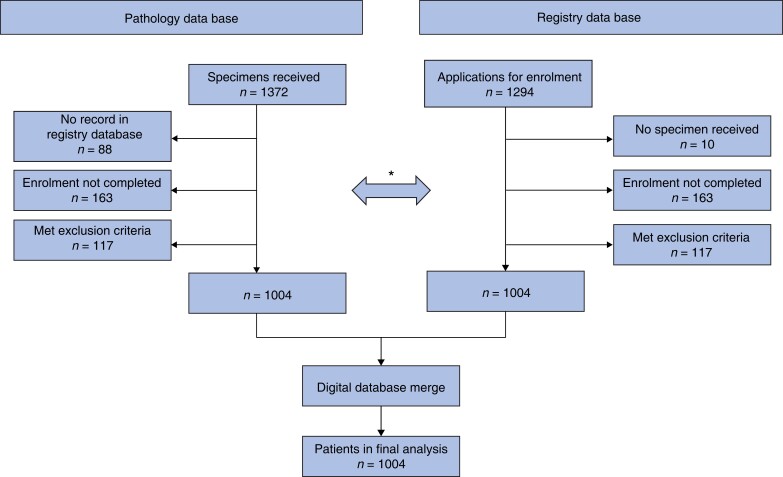
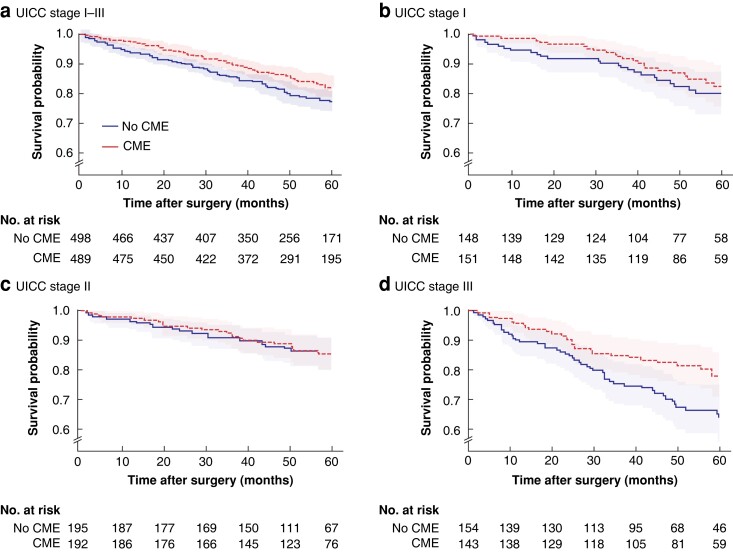
Results: A total of 1004 patients from 53 centres were recruited for the final analysis (496 CME, 508 no CME). Most operations (88.4 per cent) were done by an open approach. Anastomotic leak occurred in 3.4 per cent in the CME and 1.8 per cent in the non-CME group. There were slightly more lymph nodes found in CME than non-CME specimens (mean 55.6 and 50.4 respectively). Positive central mesenteric nodes were detected more in non-CME than CME specimens (5.9 versus 4.0 per cent). One-fifth of patients had died at the time of study with recorded recurrences (63, 6.3 per cent), too few to calculate disease-free survival (the original primary outcome), so overall survival (not disease-specific) results are presented. Short-term and overall survival were similar in the CME and non-CME groups. Adjusted Cox regression indicated a possible benefit for overall survival with CME in stage III disease (HR 0.52, 95 per cent c.i. 0.31 to 0.85; P = 0.010) but less so for disease-free survival (HR 0.66; P = 0.068). The secondary outcome (15 000 mm2 mesenteric size) did not influence survival at any stage (removal of more mesentery did not alter survival).
Conclusion: No general benefit of CME could be established. The observation of better overall survival in stage III on unplanned exploratory analysis is of uncertain significance.
© The Author(s) 2022. Published by Oxford University Press on behalf of BJS Society Ltd.
Figures
Comment in
-
Comment on: Complete mesocolic excision for right colonic cancer: prospective multicentre study.Br J Surg. 2023 Mar 30;110(4):520. doi: 10.1093/bjs/znad010. Br J Surg. 2023. PMID: 36718057 No abstract available.
-
Comment on: Complete mesocolic excision for right colonic cancer: prospective multicentre study.Br J Surg. 2023 Apr 12;110(5):614. doi: 10.1093/bjs/znad026. Br J Surg. 2023. PMID: 36723973 No abstract available.
-
Comment on: Complete mesocolic excision for right colonic cancer: prospective multicentre study.Br J Surg. 2023 May 16;110(6):734. doi: 10.1093/bjs/znad076. Br J Surg. 2023. PMID: 36935405 No abstract available.
References
-
- Hohenberger W, Weber K, Matzel K, Papadopoulos T, Merkel S. Standardized surgery for colonic cancer: complete mesocolic excision and central ligation—technical notes and outcome. Colorectal Dis 2009;11:364–365. - PubMed
-
- Bertelsen CA, Neuenschwander AU, Jansen JE, Tenma JR, Wilhelmsen M, Kirkegaard-Klitbo Aet al. . 5-year outcome after complete mesocolic excision for right-sided colon cancer: a population-based cohort study. Lancet Oncol 2019;20:1556–1565 - PubMed
-
- Bertelsen CA, Neuenschwander AU, Jansen JE, Kirkegaard-Klitbo A, Tenma JR, Wilhelmsen Met al. ; Copenhagen Complete Mesocolic Excision Study (COMES), Danish Colorectal Cancer Group (DCCG). Short-term outcomes after complete mesocolic excision compared with ‘conventional’ colonic cancer surgery. Br J Surg 2016;103:581–589 - PubMed
-
- Bertelsen CA, Neuenschwander AU, Jansen JE, Wilhelmsen M, Kirkegaard-Klitbo A, Tenma JRet al. ; Danish Colorectal Cancer Group. Disease-free survival after complete mesocolic excision compared with conventional colon cancer surgery: a retrospective, population-based study. Lancet Oncol 2015;16:161–168 - PubMed
-
- Bernhoff R, Sjovall A, Granath F, Holm T, Martling A, Buchli C. Oncological outcomes after complete mesocolic excision in right-sided colon cancer: a population-based study. Colorectal Dis 2021;23:1404–1413 - PubMed
